Prostate cancer is the common non-cutaneous cancer and the second commonest cause of cancer death in U.S. and is at present at an increasing trend in Malaysia and the Southeast Asian region. While its incidence in Malaysia is substantially lower than that in the Western hemisphere, it has been on an increasing rate even after having corrected for life expectancy.
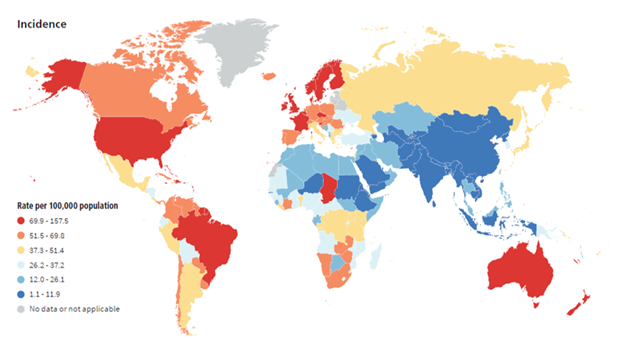
In 2022, there were an estimated 1.47 million new prostate cancer cases worldwide, making it the second most common cancer among men. The global age-standardised incidence rate (ASR) varies significantly, exceeding 100 per 100,000 in high-incidence regions like Northern/Western Europe and the Caribbean, while falling below 3 per 100,000 in parts of Asia.
Currently in the United States, the lifetime risk of being diagnosed with prostate cancer is approximately 1 in 8 men (roughly 12.8% to 13%), while the lifetime risk of dying from the disease is about 2% to 2.6%, or roughly 1 in 39 to 1 in 49 men. Prostate cancer is highly survivable, particularly when detected early, with a 5-year relative survival rate over 98% compare this with the estimates for the year 2000 which indicate a worldwide prostate cancer incidence of 542,990 new cases, 204,313 of whom have died. An estimated 220,900 new cases of prostate cancer were diagnosed in the United States in 2003, and 28,900 men died of the disease during that year. The lifetime risk for diagnosis of prostate cancer is 17% in the United States, and the risk for dying from prostate cancer is 3.4%.
Incidence of prostate cancer worldwide, age-standardised using world standard population
Malaysia
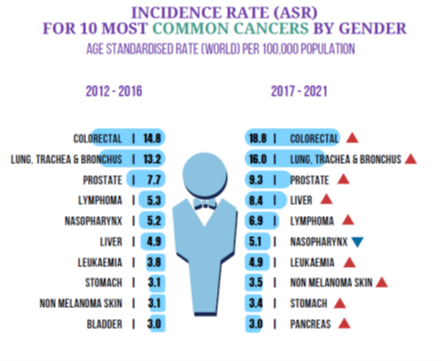
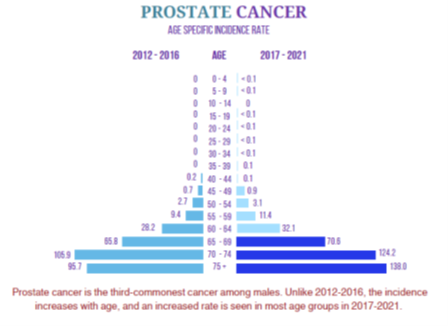
Prostate cancer is the third most common cancer among men in Malaysia, with an increasing incidence rate and a high prevalence of late-stage diagnosis
Age-Standardized Rate (ASR):
The age-standardised incidence rate of prostate cancer in Malaysia has risen, reported at roughly 9.3 per 100,000 men in 2021, up from 7.7 in 2016. Other recent studies (2022 data) estimate the overall ASR to be around 12.9 per 100,000 population.
Incidence Trend: The incidence is increasing in Malaysia. Prostate cancer is the poster-child example of a scrutiny-dependent cancer – meaning the more one screens, the more number of cancers will be detected.
Not all prostate cancers are lethal; many are slow-growing (indolent) and never cause symptoms or death, leading to the saying that most men die WITH prostate cancer rather than OF it.

SUMMARY OF THE MANAGEMENT OF PROSTATE CANCER:
Key Guidelines and Recommendations:
Screening: Asymptomatic men should discuss screening with doctors around age 50 (earlier for high-risk, e.g., Black men or family history), and discuss the pros and cons of PSA screening.
Symptoms: Early-stage symptoms are often absent but can include frequent urination, trouble starting urination, or blood in the urine/semen. Patients who are symptomatic with lower urinary tract symptoms mandates a PSA test and rectal examination to assess the prostate.
Diagnosis: Diagnosis is confirmed via biopsy and staging (I–IV) using MRI, CT, or bone scans.
A prostate biopsy is a medical procedure used to remove small samples of tissue from the prostate gland to be examined under a microscope. It is currently the only definitive way to diagnose prostate cancer.
When is a Biopsy Recommended?
Because the PSA test cannot reliably distinguish between a “tiger” (aggressive cancer) and a “pussycat” (slow-growing cancer), major health organisations generally recommend that men have a thorough discussion with their doctor about the trade-offs before getting tested
Urologists usually recommend a biopsy if initial screening tests suggest a problem:
- High PSA Levels: A prostate-specific antigen (PSA) blood test shows higher-than-normal levels for your age.
- Abnormal Rectal Exam: A digital rectal exam (DRE) reveals lumps or hard areas on the prostate.
- Suspicious MRI: An MRI scan shows areas that appear potentially cancerous.
- Active Surveillance: You have already been diagnosed with low-risk cancer and need regular monitoring.
Prostate Biopsy:
Prostate biopsy is used to take samples of prostatic tissue and send them for histopathological confirmation to diagnose prostate cancer. Prostate biopsy be done either by transrectal, transperineal or MRI Ultrasound-fusion prostate biopsy.
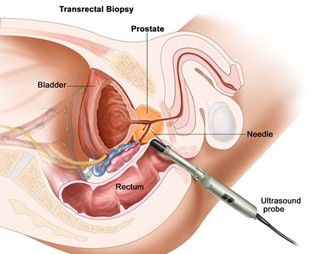
Transrectal prostate biopsy:
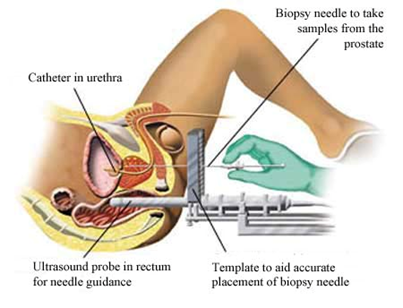
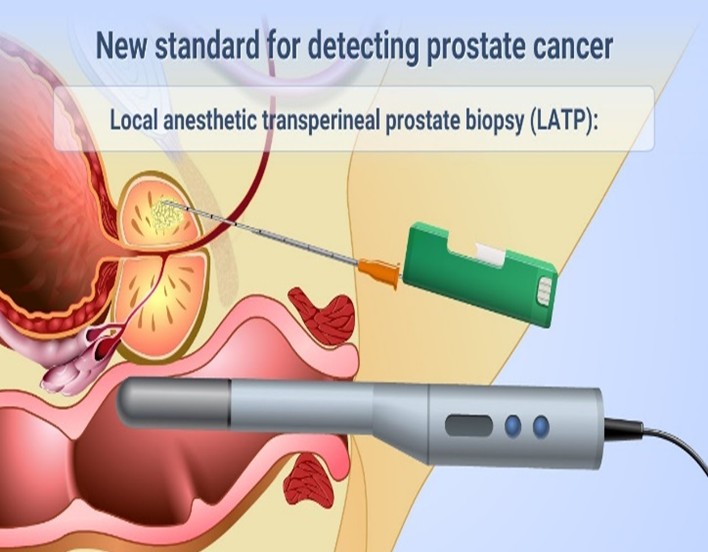
Transperineal prostate biopsy
MRI ultrasound-fusion prostate biopsy
Types of Prostate Biopsy Procedures
| Type | |||
| How It’s Done | Common Settings | ||
| Transrectal (TRUS) | Needle passes through the wall of the rectum. Guided by ultrasound. | Often done in a doctor’s office with local anesthesia. | |
| Transperineal | Needle passes through the skin (perineum) between the scrotum and anus. Lower infection risk. | Can be done under local or general anesthesia in a clinic or hospital. | |
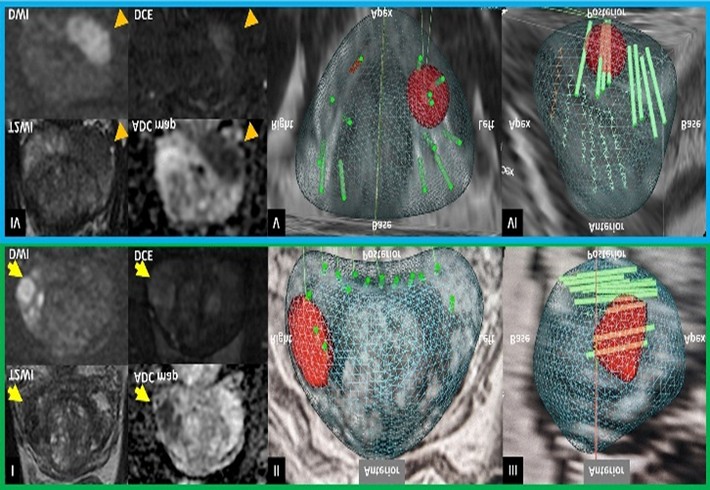
| MRI-Ultrasound Fusion | Combines MRI and ultrasound images to create a 3D map, allowing for targeted sampling of suspicious areas. | Performed in hospitals or specialized clinics. | |
IMAGING:
Imaging for prostate cancer focuses on three areas: localisation within the gland, local staging (nearby spread), and distant staging (metastasis).
1. Diagnosis and Local Staging (T-Stage)
- Multiparametric MRI (mpMRI): The gold standard for detecting tumors within the prostate and assessing extracapsular extension. It combines anatomical (T2-weighted) and functional (DWI and DCE) imaging.
- Transrectal Ultrasound (TRUS): Primarily used to guide biopsy needles rather than for definitive staging, though it helps measure prostate volume.
2. Assessing Spread to Nodes and Bones (N & M-Stage)
- PSMA PET/CT: The most sensitive and specific modern technique. It uses a radioactive tracer that binds to Prostate-Specific Membrane Antigen to find tiny clusters of cancer cells throughout the body.
- Bone Scan (Technetium-99m): Used specifically to detect bone metastases, typically indicated if PSA levels are high or the Gleason score is aggressive.
- CT Scan (Abdomen/Pelvis): Used to check for enlarged lymph nodes or spread to visceral organs (liver/lungs), though it is less sensitive than PET for early spread.
- Whole-Body MRI (WBMRI): An alternative for detecting bone and marrow involvement without using radiation.
Risk stratification:
Prostate cancer management, unlike other cancers, focuses on risk-stratified management, using PSA testing and Digital Rectal Examination (DRE) for early detection, generally starting at age 50.
Risk-stratified assessment of prostate cancer is critical for determining the appropriate intensity of treatment, as it aligns management with the potential for disease progression. This approach, commonly using NCCN or D’Amico classification systems, categorises newly diagnosed, non-metastatic prostate cancer into groups ranging from very low to high risk, based on PSA levels, biopsy Grade Group (Gleason score), and clinical stage (T-stage).
Treatment strategies for prostate cancer are highly individualised and based on a combination of tumor characteristics, patient health, and personal preferences. The primary goal is to balance effective cancer control with the management of potential side effects, such as urinary incontinence and erectile dysfunction.
Age and life expectancy are important parameters in deciding treatment strategy.
Younger men may be offered more aggressive treatment, while older men with slow-growing tumors might be advised to avoid immediate treatment.
Risk Groups and Typical Treatment Strategies
- Very Low / Low Risk: Often managed with active surveillance (closely monitoring with PSA tests, biopsies, and imaging). Treatment is often avoided to prevent overtreatment of indolent disease.
- Intermediate Risk: Favorable vs. unfavorable intermediate risk is determined by the percentage of high-grade cancer and PSA levels. Treatments commonly include surgery (radical prostatectomy) or radiation therapy (EBRT or brachytherapy).
- High Risk / Very High Risk: Usually requires combined therapies, such as radiotherapy with long-term androgen deprivation therapy (ADT), or surgery with potential adjuvant treatment
Treatment for localised disease includes active surveillance, radical prostatectomy, or radiotherapy, while advanced stages are managed with hormone therapy, PARP inhibitors, or chemotherapy.
TREATMENT
Management of prostate cancer is categorised by the extent of the disease, focusing on curative intent for early stages and life extension or symptom control for advanced stages.
Localised Disease
Here the cancer is confined to the prostate. The primary goal is a cure while minimizing side effects.
- Active Surveillance: For low-risk cases, involves regular monitoring (PSA tests, biopsies) to delay treatment until necessary.
- Radical Prostatectomy: Surgical removal of the prostate; often preferred for younger, healthy patients.
- Radiation Therapy: External beam radiation (EBRT) or brachytherapy (seeds), sometimes combined with short-term hormone therapy.
Locally Advanced Disease
The cancer has spread just outside the prostate capsule or into seminal vesicles.
- Multimodal Therapy: Usually a combination of long-term Androgen Deprivation Therapy (ADT) and radiation therapy.
- Surgery: Radical prostatectomy with extensive lymph node dissection may be an option for select patients.
- Intensification: Recent 2026 guidelines often recommend adding agents like abiraterone to the standard ADT / radiation mix to improve survival.
Metastatic Disease
Here the cancer has spread to bones, lymph nodes, or other organs.
Hormone Therapy / Androgen Deprivation therapy (ADT): This is the standard treatment for advanced or metastatic castration-sensitive and resistant prostate cancer (mCRPC).
Systemic Doublet vs Triplet Hormonal Therapy:
- The current gold standard is for doublet hormonal therapy involving ADT +/- an androgen receptor pathway inhibitor (ARPI) (e.g., abiraterone, enzalutamide) OR docetaxel (chemotherapy).
- In fit patients, this involves triplet therapy consisting of ADT + an androgen receptor pathway inhibitor (ARPI) (e.g., abiraterone, enzalutamide) + docetaxel (chemotherapy).
PARP Inhibitors: Used for recurrent mCRPC in patients with specific genetic mutations (BRCA1, BRCA2, or ATM).
Multidisciplinary Approach: Management plans are typically created by multidisciplinary experts.
Radioligand Therapy: Treatments like Lutetium-177 PSMA-617 are used for patients who progress despite initial hormone therapy.
Palliative Care: Focused on bone health (bisphosphonates) and pain management to maintain quality of life.
Detailed individual treatments and the various controversies of prostate cancer treatment will be detailed in subsequent follow up articles.