Beyond Radical Prostatectomy (RP) and Radiotherapy (RT), several focal therapy modalities have emerged. As of 2026, Focal Therapy in localised prostate cancer is considered a non-standard investigational option for clinically localised low and intermediate risk prostate cancer patients who wish to avoid the side effects of radical surgery or radiation.
It is specifically aimed at patients with localised, low- or intermediate-risk prostate cancer, particularly those with Gleason Score 7 (3+4) tumors that are well-localised, where the goal is to treat the cancer while preserving surrounding tissue.
Focal therapy in prostate cancer is considered an emerging, minimally invasive treatment modality designed to destroy specific, cancerous areas within the prostate (index lesions) while sparing surrounding healthy tissue. They require ongoing review, entrance into clinical trials and a prospective trial registry. Patients must be informed that it is a non-standard investigational option currently undergoing clinical trials.
Robust prospective trials reporting standardised 15-year oncological outcomes are needed in patients with clinically significant cancers before unrestricted recommendations in support of focal therapy for routine clinical practice can be made.
Currently, focal therapy using HIFU, cryotherapy, IRE and other various focal therapy modalities should be performed within the context of a prospective registry.
All other ablative modalities and treatment strategies should only be offered in a well-designed prospective trial setting.
Whole gland treatments using cryosurgery and HIFU were investigated as a replacement for surgery or radiotherapy, with only limited success.
FDA Clearance of HIFU and Irreversible Electroporation (IRE / NanoKnife)
U.S. FDA approval for HIFU in the U.S. (achieved in 2015 for tissue ablation, not specifically for BPH or cancerous tumor clearance) was delayed for nearly a decade due to a combination of clinical, regulatory, and financial challenges.
FDA clearance for the use of HIFU in clinical practice is for the ablation of prostate tissue, rather than for the specific treatment of prostate cancer
While FDA approval in 2015 was for the general “ablation of prostate tissue”, this technical approval enables clinicians to use it as a targeted tool for removing diseased tissue (cancer) within the prostate.
Similarly, IRE / NanoKnife System received FDA 510(k) clearance in late 2024 for the ablation of prostate tissue, rather than for the specific treatment of prostate cancer.
Rationale of Focal Therapy in Clinically Localized Prostate Cancer
The central philosophy of these treatments is the “Index Lesion” theory: destroying the primary tumor while sparing the rest of the prostate to preserve sexual and urinary function.
Reduced Morbidity: Radical therapies are associated with high rates of erectile dysfunction (24–90%), urinary incontinence (2–72%), and rectal toxicity. Focal therapy seeks to achieve oncological control with significantly fewer complications.
Index Lesion Hypothesis: Evidence suggests that in multifocal disease, the highest-grade tumour (index lesion) is primarily responsible for cancer progression and metastasis. Treating this lesion while monitoring the rest of the gland is considered sufficient for many patients.
Overtreatment Mitigation: Many men are diagnosed with low- or favorable intermediate-risk disease that may not require whole-gland treatment. Focal therapy allows targeted intervention, reducing the psychological burden of active surveillance and the harms of immediate radical treatment.
Advancements in Imaging: Improved detection via multiparametric magnetic resonance imaging (mpMRI) and PSMA-PET/CT allows precise localisation of the index tumor for targeted ablation.
Types of Focal Therapy (Energy Modalities)
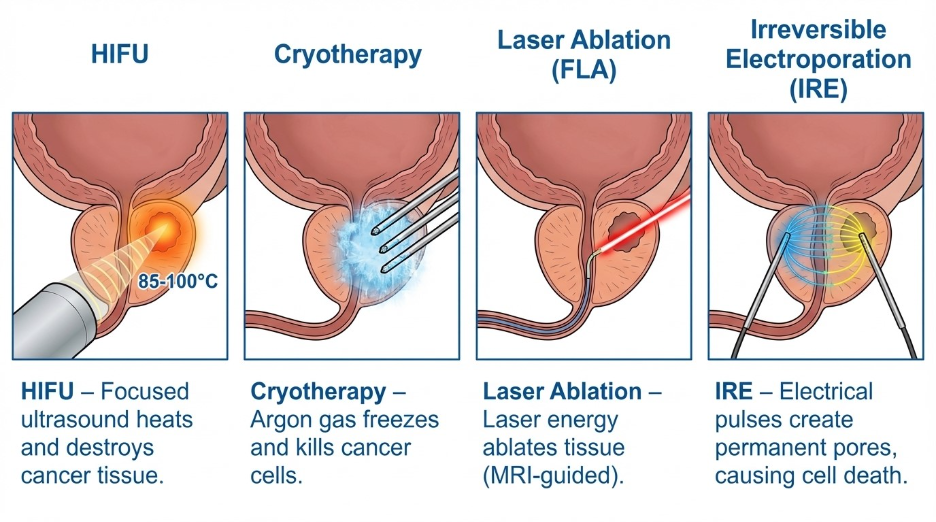
Focal therapies include HIFU, Cryotherapy, TULSA (Transurethral Ultrasound Ablation), Focal Laser Ablation (FLA), Photodynamic therapy (PDT) and Irreversible Electroporation (IRE).
Various ablative techniques are used, with HIFU and Cryotherapy being the most established.
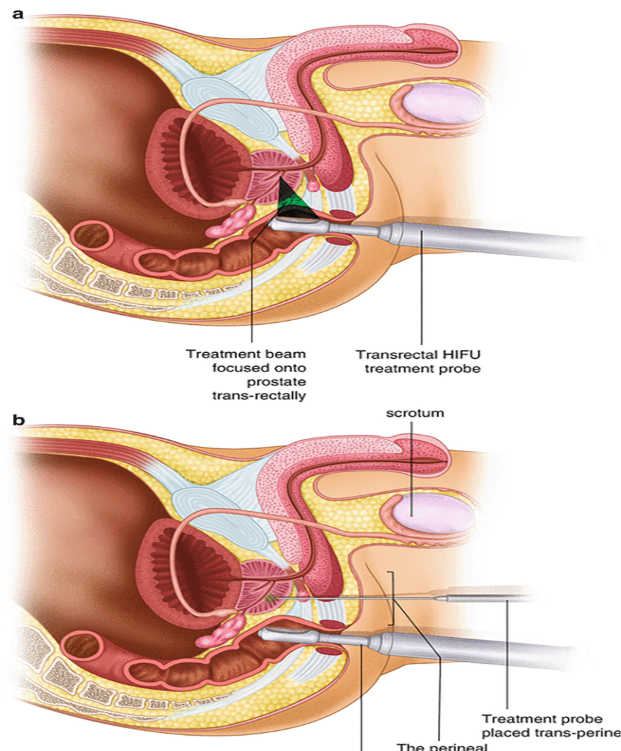
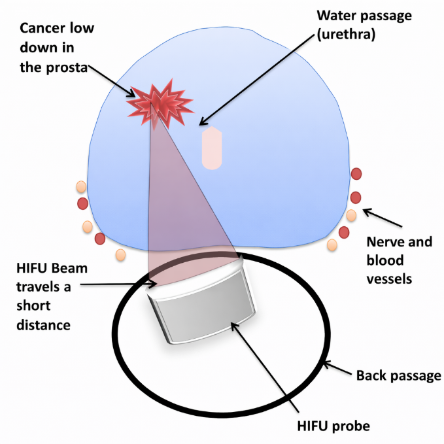
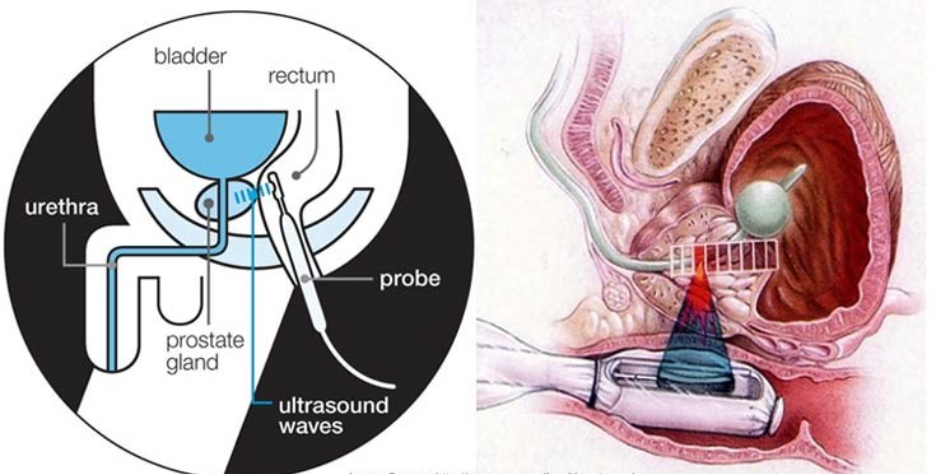
High-Intensity Focused Ultrasound (HIFU): Uses ultrasound waves to generate heat (>80C) to destroy tissue, usually via a rectal probe.
Cryotherapy (Cryoablation): Uses freezing temperatures (<30C) applied via transperineal needles to cause cell necrosis.
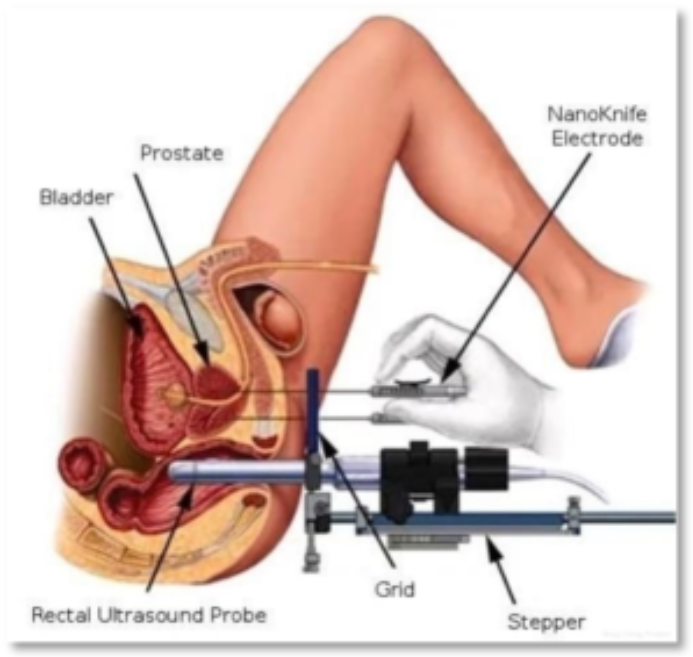
Irreversible Electroporation (IRE / NanoKnife): A non-thermal technique using high-voltage, low-energy electrical pulses to trigger cell death (apoptosis) while sparing connective tissue and critical structures.
Focal Laser Ablation (FLA / ILT): Employs laser fibers for thermal destruction (photothermal effect) of cancer cells under MRI guidance.
Vascular-Targeted Photodynamic Therapy (VTP/Tookad): Uses intravenous photosensitizing agents activated by light to induce vascular shutdown, resulting in tissue necrosis.
Transurethral Ultrasound Ablation (TULSA): A newer technique using an ultrasound device within the urethra to treat prostate tissue under MRI monitoring.
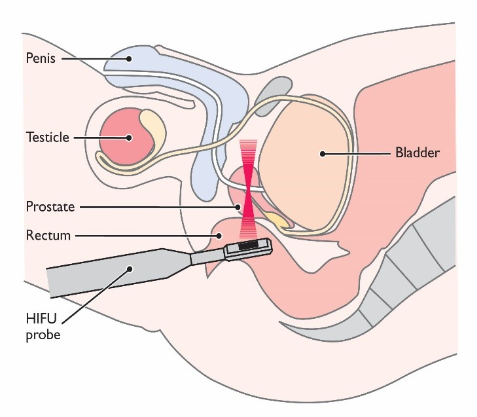
1. High-Intensity Focused Ultrasound (HIFU)
- Mechanism: Uses a transrectal probe to focus ultrasound waves on a specific point in the prostate, heating the tissue to over 80°C and causing thermal necrosis.
- Efficacy: The 2026 HIFI Study reported that focal HIFU is non-inferior to radical prostatectomy regarding “salvage treatment-free survival” (approx. 90% at 30 months).
HIFI TRIAL: HIFU VS RADICAL PROSTATECTOMY FOR LOCALIZED PROSTATE CANCER IN 3328 CASES. FINAL RESULTS
The HIFI trial is the first prospective study comparing HIFU vs RP as primary treatment for localised prostate cancer. Salvage therapy-free survival after HIFU was not inferior to that reported after RP at the pre- planned 30-month follow-up. Patient-reported outcomes showed a significant lower negative impact of HIFU on functional outcomes such as urinary continence and erectile function.
- Verdict: Now a first-line option in many centers for focal lesions. It has significantly lower rates of incontinence and erectile dysfunction compared to RP. However, long-term (10+ years) data still needs catching up to surgery
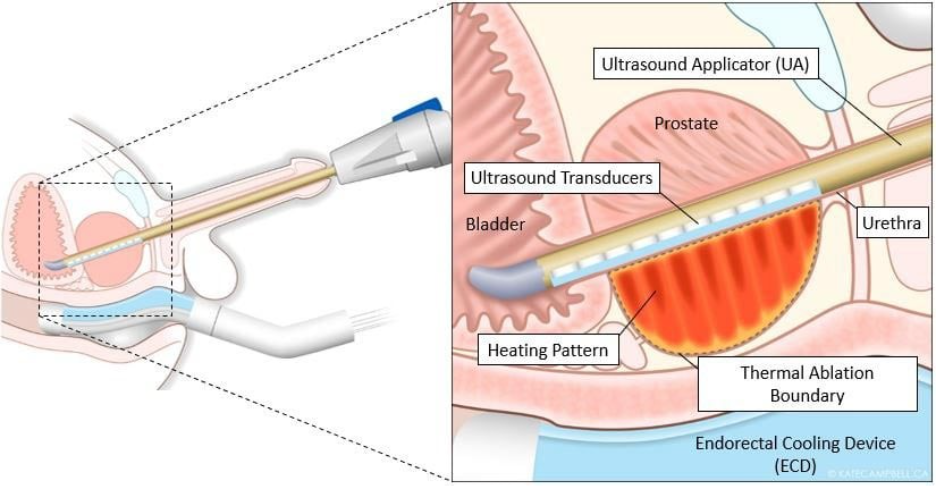
2. TULSA-PRO (Transurethral Ultrasound Ablation)
- Mechanism: A newer variant where ultrasound energy is delivered from inside the urethra rather than the rectum. It is performed inside an MRI scanner for real-time temperature monitoring.
- Significance: It is more precise than standard HIFU and can treat larger areas or even the whole gland.
- Verdict: Highly effective for functional preservation, but access is currently limited to high-volume specialised centres.
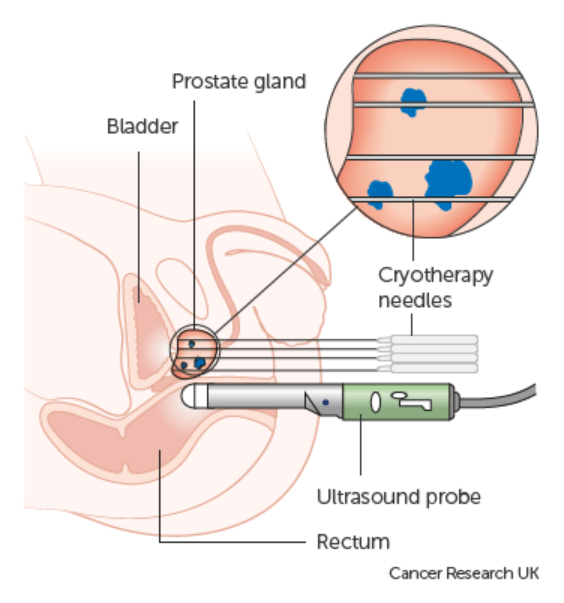
3. Cryotherapy (Cryoablation)
- Mechanism: Insertion of “cryoneedles” into the prostate to circulate liquid nitrogen or argon gas, creating an “ice ball” that freezes and kills the cancer cells.
- Indication: Often used for patients who cannot tolerate surgery or as a salvage treatment if radiation therapy has failed.
- Verdict: Well-established with good short-term results. The risk of erectile dysfunction is higher than HIFU but lower than radical surgery.
4. Irreversible Electroporation (NanoKnife / IRE)
- Mechanism: Unlike thermal methods, IRE uses ultra-short, high-voltage electrical pulses to create permanent “nanopores” in the cell membrane, leading to cell death.
- Significance: It is “non-thermal,” meaning it does not use heat or cold. This allows it to be used near critical structures like nerves and blood vessels without damaging them.
- Verdict (2026): Considered a breakthrough for tumors located near the prostate edge (apex or base). Early data shows about 75% of patients remain free from radical treatment at 5 years.
5. Comparison of Modalities
| Modality | Energy Source | Main Advantage | Primary Risk |
| HIFU | Heat (Sound) | No needles; strong data | Urethral stricture |
| TULSA | Heat (MRI-Guided) | Real-time precision | Specialized equipment needed |
| Cryotherapy | Cold (Ice) | Effective for salvage | Tissue sloughing |
| NanoKnife | Electricity | Preserves nerves/vessels | Requires general anesthesia |
Focal modalities used based on site of focal tumor:
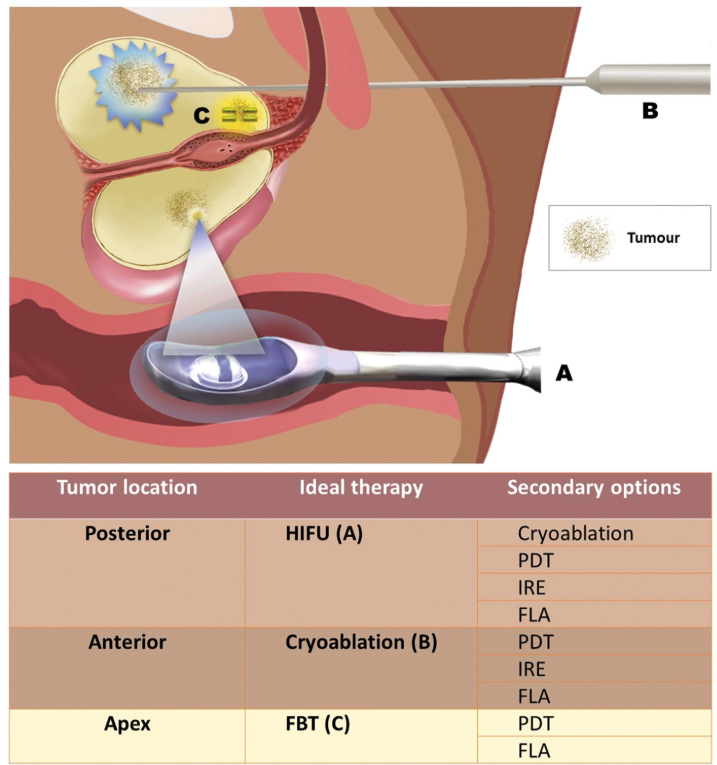
FBT = Focal Brachytherapy
NOTE: Total prostate gland ablation with HIFU is currently not considered standard first-line treatment and is often used for prostate cancer recurrences.
Experts are studying long-term outcomes using HIFU focal therapy and starting clinical trials to improve energy inside the prostate gland as well as ways to reduce disease recurrence. More long term studies are required.
Controversies on the short term and long-term results of focal therapy modalities for prostate cancer
The controversy surrounding focal and minimally invasive therapies (MITs) for prostate cancer centers on the “Trade-off Principle”: Functional Preservation vs. Oncological Certainty.
While major trials like the 2024–2026 updates to the HIFI and the PART study (Prostate cancer: Actively Researching Targeted therapy study) have clarified their role, significant debate remains regarding their long-term reliability compared to the “Gold Standards” of surgery and radiation.
1. High-Intensity Focused Ultrasound (HIFU)
Short-Term Results (0–2 Years)
- Efficacy: High rates of “negative biopsy” in the treated area (approx. 80–90%).
- Functional Outcomes: Excellent. Most men maintain urinary continence and erectile function immediately post-procedure.
- Controversy: The “Post-HIFU PSA” is difficult to interpret. Since part of the healthy prostate remains, PSA never drops to zero, leading to significant patient anxiety.
Long-Term Results (5–10+ Years)
- Efficacy: About 20–30% of patients require a “salvage” radical treatment (surgery or radiation) within 5 to 8 years.
- Controversy: Critics argue that HIFU merely “kicks the can down the road.” Proponents argue that delaying radical treatment by 7 years preserves 7 years of high-quality life, which is a success in itself.
2. Irreversible Electroporation (NanoKnife / IRE)
Short-Term Results
- Efficacy: Highly effective at destroying the visible “index lesion.”
- Safety: IRE is uniquely safe for tumors near the urethra or neurovascular bundles because it doesn’t use heat.
- Controversy: It is highly dependent on the surgeon’s ability to map the tumor accurately using MRI-Ultrasound fusion.
Long-Term Results
- Efficacy: Data is still maturing. Early 5-year results suggest cancer control rates are comparable to HIFU, but the “Field Effect” controversy remains – the concern that untreated areas of the prostate may already harbor microscopic cancer that IRE missed.
3. The “Global Controversy” Matrix
| Controversy Type | The “Focal” Argument | The “Radical” Argument |
| The Index Lesion | 90% of a cancer’s threat comes from the largest (index) nodule. Kill that, and the patient is safe. | Prostate cancer is multifocal. Small, invisible tumors left behind will eventually turn aggressive. |
| Salvage Surgery | If HIFU fails, we can still do surgery or radiation later. | Surgery after HIFU or Cryotherapy is significantly harder and has higher complication rates due to scarring. |
| Cost-Effectiveness | Fewer hospital days and fewer complications save the healthcare system money. | The high cost of specialized equipment and the need for frequent follow-up MRIs/biopsies offset the initial savings. |
| The “Wildcard” | PSMA-PET now allows us to see exactly where the cancer is, making focal therapy safer than ever. | Even PSMA-PET cannot see clusters of cancer smaller than 2-3mm. |
4. Efficacy Verdict by Modality (2026)
- HIFU: Verdict: Strong. Best for “posterior” tumors (near the rectum). Most established long-term data among MITs.
- TULSA-PRO: Verdict: Emerging. Excellent for whole-gland or large-volume ablation with minimal recovery time.
- Cryotherapy: Verdict: Specialized. Highly effective but generally carries a slightly higher risk of erectile dysfunction than HIFU; excellent for salvage after radiation failure.
- NanoKnife (IRE): Verdict: Precision Tool. The preferred choice for tumors at the apex of the prostate where preserving the sphincter is critical.
Summary of Results
- Short-Term: Focal therapies are clear winners for Quality of Life (QoL).
- Long-Term: Radical Prostatectomy remains the winner for “Cancer-Free Survival,” though the gap is narrowing as mapping technology (like AI-assisted MRI) improves.
Urologists would typically recommend these modalities only for “Intermediate-Risk” patients (Gleason 3+4) who are highly motivated to avoid the side effects of radical surgery. The “Success” of these treatments is increasingly defined not just by the absence of cancer, but by the “Trifecta”: Cancer control, urinary continence, and potency.
Informed decisions over QOL issues versus cancer control and survival rates of prostate cancer treatment needs to be an important decisive factor in minimally invasive treatment of localised prostate cancer.
The “Functional Strategy” for 2026
In practice, a PSMA-PET scan to “double-check” a candidate is necessary for focal therapy. If the PSMA-PET shows only one bright spot that matches the MRI, focal therapy is a strong candidate. However, if the PSMA-PET “lights up” in areas the MRI missed, the recommendation will shift immediately to Radical Prostatectomy to avoid leaving cancer behind.
Current Role & Status
- Gold Standard: Radical prostatectomy (surgery) and radiation therapy remain the primary benchmarks due to extensive long-term survival data.
- Investigative / Alternative: While FDA-approved for prostate tissue ablation, HIFU is often categorized as an alternative for patients seeking to bridge the gap between active surveillance and radical surgery. It is increasingly used in focal therapy to target specific lesions while sparing surrounding healthy tissue.
HIFU is a viable choice for patients with low-to-intermediate risk localised cancer who prioritise preserving quality of life (continence and sexual function). However, most clinical guidelines still emphasize that it lacks the multi-decade longitudinal data associated with traditional standards.
Comparison Of Active Surveillance, Radical Prostatectomy, Radiotherapy And Hifu For Low Risk Prostate Cancer
For men with low-risk prostate cancer, managing the disease requires balancing cancer control with maintaining quality of life. The optimal choice often depends on your overall health, age, and personal preferences regarding potential side effects.
| Feature | Active Surveillance | Radical Prostatectomy | Radiotherapy | HIFU (Focal Therapy) |
| Description | Close monitoring with routine PSA tests, MRIs, and biopsies. Treatment is only given if tests show the cancer is progressing. | Surgical removal of the entire prostate gland and seminal vesicles. | Use of high-energy rays (external beam or brachytherapy) to kill cancer cells. | Targeted ultrasound energy focused to destroy only the tumor while sparing the rest of the prostate. |
| Primary Goal | Avoid the side effects of immediate treatment while ensuring cancer doesn’t spread. | Completely eradicate the cancer from the prostate. | Destroy cancer cells while avoiding surgery. | Provide a middle-ground by treating the cancer with minimal damage to healthy surrounding tissues. |
| Treatment Frequency | Intermittent (repeated biopsies and tests over time). | One-time procedure. | Usually given daily over several weeks, or as a one-time implant (brachytherapy). | One-time procedure, though a repeat may be needed if new lesions arise. |
| Common Side Effects | None from treatment; potential anxiety over living with untreated cancer. | Higher risk of urinary incontinence and erectile dysfunction. | Higher risk of bowel symptoms (e.g., urgency, bleeding), erectile dysfunction, and fatigue. | Lower risk of incontinence and erectile dysfunction compared to radical therapies. |
| Long-Term Cancer Control | Same 10-year survival rate as surgery or radiation for low-risk, but higher chance of requiring treatment later. | Lowest risk of local cancer progression. | Excellent cancer control; comparable to surgery for localized disease. | Good short to mid-term control, but longer-term (10+ year) data is still emerging. |
| Recovery / Lifestyle Impact | Immediate return to normal life, though requires lifestyle adjustments for routine hospital visits. | Takes 1 to several months to regain full urinary control; hospital stay is usually 1-3 days. | Minimal disruption during treatment days; side effects may develop gradually over weeks/months. | Quick recovery; typically outpatient or 1-day hospital stay with a catheter for a few days. |
Summary Points
Active Surveillance is generally the gold-standard recommendation for low-risk prostate cancer, successfully deferring or entirely avoiding the morbidity of aggressive treatments without compromising survival.
Radical Prostatectomy and Radiotherapy offer definitive, whole-gland cures but carry higher lifelong risks of sexual and urinary side effects.
HIFU serves as a focal or partial gland therapy, bridging the gap by offering active treatment while preserving sexual and urinary function better than radical options.
Comparison Of Radical Prostatectomy, Radiotherapy And HIFU For Low Risk Prostate Cancer
For low-risk prostate cancer, treatment options are increasingly focused on balancing high cure rates with quality-of-life preservation. While radical prostatectomy (RP) and radiotherapy (RT) remain standard, High-Intensity Focused Ultrasound (HIFU) is a growing, less-invasive alternative, often used for focal therapy.
Low-Risk Prostate Cancer Treatment Comparison (As of 2026)
| Feature | Radical Prostatectomy (RP) | Radiotherapy (RT/SBRT) | HIFU (Whole Gland or Focal) |
| Approach | Surgical removal of prostate | Radiation energy to kill cells | Targeted thermal ablation (heat) |
| Invasiveness | High (Minimally invasive or open) | Low | Low (Transrectal probe) |
| Treatment Area | Whole gland | Whole gland (+/- lymph nodes) | Focal (part) or Whole gland |
| Hospital Stay | Usually 1–2 days | Outpatient | Outpatient |
| Recovery Time | 4–6 weeks | Minimal (potential fatigue) | 1–2 weeks |
| Oncological Control | Excellent (long-term data) | Excellent (long-term data) | Very good (comparable to RP/RT at 5–7 years) |
| Incontinence Risk | Moderate to High | Low (primarily urgency) | Low |
| Erectile Dysfunction | High (60–80% for non-nerve sparing) | Moderate (40-60% over time) | Lower than RP/RT |
| Rectal Side Effects | Low | Low to Moderate (bowel habits) | Very Low |
| Salvage Options | Yes (Radiation/HIFU) | Yes (Surgery/HIFU) | Yes (Surgery/Radiation) |
Key Considerations for 2026 Treatment Selection for Low Risk Prostate Cancer
Active Surveillance (AS): AS is the preferred “standard of care” for true low-risk prostate cancer, allowing men to defer treatment entirely until necessary, as early intervention may not improve survival in this group.
Radical Prostatectomy (RP): Offers immediate removal of the cancer and pathological staging (pathologist examines the whole gland). It is associated with higher risks of urinary leakage and erectile dysfunction compared to the other methods.
Radiotherapy (RT/SBRT): A non-invasive approach with comparable long-term survival rates to surgery for low-risk disease. Modern techniques like SBRT have reduced side effects, though bowel urgency can occur.
HIFU: Frequently used as a “middle ground,” offering a “focal” option (treating only the tumor rather than the whole gland) which results in fewer side effects – specifically preserving urinary continence and sexual function better than radical approaches. However, long-term (>10 years) data is less established than RP or RT.
Comparison Of Radical Prostatectomy, Radiotherapy And HIFU For Intermediate Risk Prostate
Based on data from 2024–2026, the following table compares radical prostatectomy (RP), radiotherapy (RT), and High-Intensity Focused Ultrasound (HIFU) for intermediate-risk prostate cancer.
Comparison Table: Intermediate-Risk Prostate Cancer Treatments
| Feature | Radical Prostatectomy (RP) | Radiotherapy (RT) | HIFU (Focal Therapy) |
| Approach | Surgical removal of the entire prostate gland. | External beam (EBRT) or Brachytherapy to kill cancer cells. | Focused ultrasound beams to ablate specific tissue. |
| Primary Goal | Complete removal (Curative). | Destruction of tissue (Curative). | Focal/Targeted (Spare healthy tissue). |
| Oncological Efficacy | High; established long-term survival rates. | High; often combined with ADT for intermediate risk. | Good, but higher risk of recurrence than whole-gland. |
| 5-Yr Cancer Control | ~85–90%+ (Depends on study/risk). | ~85–90%+ (Comparable to RP). | ~45–88% (Variable, often lower). |
| Urinary Continence | High risk of short-term leakage; improved long-term. | Lower risk of incontinence, higher risk of frequency/urgency. | Best preservation; lower risk of incontinence. |
| Erectile Function | Significant decline, high ED risk. | Gradual decline over time. | Best preservation, lower ED risk. |
| Bowel/Rectal Side Effects | Very Low. | High risk (bleeding, urgency). | Low. |
| Hospital Stay | Usually 1–2 days (Robotic). | Outpatient (no surgery). | Outpatient (or 1-day stay). |
Key Takeaways for Intermediate Risk Prostate Cancer
Radical Prostatectomy (RP): Often considered the standard for younger, active men with intermediate-risk disease to ensure full cancer removal, but carries the highest risk of incontinence and erectile dysfunction.
Radiotherapy (RT): An effective alternative to surgery, particularly with modern SBRT or brachytherapy. It avoids immediate incontinence but increases long-term risk of bowel issues.
HIFU (Focal Therapy): Emerging as a favorable option for patients with unilateral (one-sided) intermediate-grade prostate cancer who are highly motivated to preserve sexual and urinary function. It has a much lower side-effect profile but a higher risk of needing a second, “salvage” treatment later.
Note: The 30-month Salvage Treatment Free Survival (STFS) rate has been reported as higher for HIFU (89.8%) compared to RP (86.2%) in specific comparative studies
Key Considerations In 2026
Diagnostics: Advanced, multi-parametric MRI and PSMA PET scans are crucial for identifying candidates for focal therapy.
Selection: Focal therapy is best suited for favorable intermediate-risk disease, often within clinical trials.
Key Guideline Consensus On HIFU (As Of 2026):
As of early 2026, High-Intensity Focused Ultrasound (HIFU) for prostate cancer is generally considered investigative or an emerging, non-standard alternative in the United States, rather than part of the established standard of care.
- Investigational Status: The AUA states that whole-gland or focal ablation (including HIFU) for localised prostate cancer remains investigational due to a lack of high-quality comparative data against standard care (e.g., radical prostatectomy, radiotherapy, and active surveillance).
- Recommendation Restriction: The EAU advises that HIFU should only be offered within the context of clinical trials or well-designed prospective cohorts.
- NCCN Position: The NCCN Guidelines generally recognise HIFU primarily as a salvage option for non-metastatic recurrence after definitive radiation, rather than as a standard primary therapy.
- Patient Counseling: Clinicians are advised to inform patients that HIFU is not considered a standard care option.
While FDA-cleared for prostate tissue ablation, HIFU is not recognized by these major guidelines as a standard alternative to conventional curative treatments.
Current Role Of Focal Therapy In Prostate Cancer Treatment (2026)
High-intensity focused ultrasound (HIFU) is still primarily categorised as investigational for the primary treatment of clinically localized prostate cancer in 2026.
This is because there is a lack of high-quality data comparing them to standard care like surgery or radiation
HIFU is more established as a “salvage” option for patients whose cancer has returned after radiation, though even in this context, it is often viewed as an emerging alternative to more invasive salvage surgery
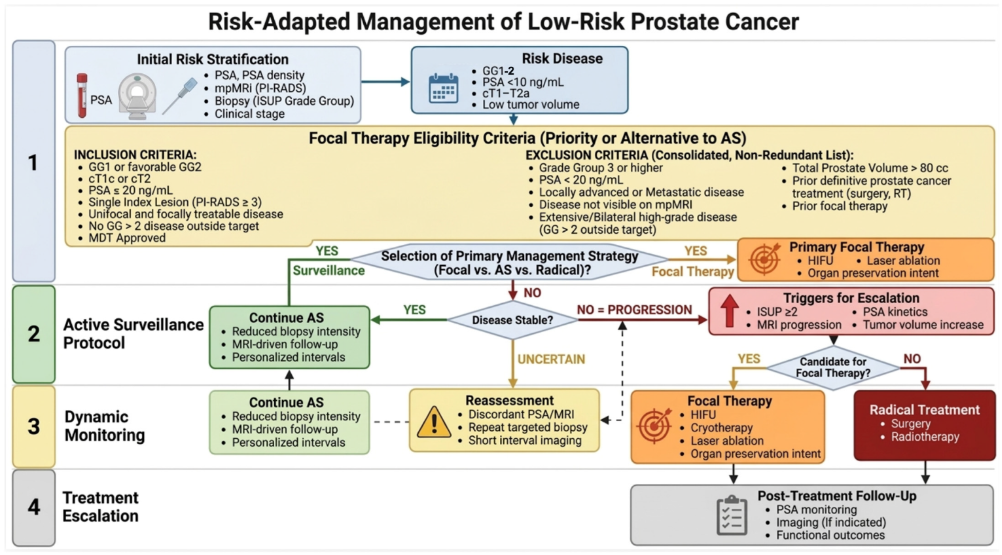
Patient Selection: The optimal candidate has localized intermediate-risk disease (ISUP Grade 2-3) with a well-defined index lesion visible on mpMRI.
Clinical Status: While considered promising, focal therapy is not yet deemed the standard of care for all patients. It is generally recommended that Focal therapy be offered within a clinical trial setting or well-designed prospective registries.
Salvage Treatment: Focal therapy is increasingly used as a “salvage” option for men whose cancer recurs after initial radiotherapy, offering comparable survival to radical salvage surgery with significantly fewer complications (9–24 times lower odds of complications).
Functional Outcomes: Studies indicate >90% preservation of urinary continence and significant preservation of erectile function compared to radical prostatectomy.
Follow-up: Because not all prostate tissue is treated, rigorous follow-up with serial PSA tests, mpMRI, and targeted biopsies is required
Key Guideline Consensus on Irreversible Electroporation (IRE / NanoKnife) – as of 2026:
The NanoKnife System (which uses IRE technology) received FDA 510(k) clearance in December 2024 specifically for the ablation of prostate tissue, and not specifically prostate cancer treatment.
According to the National Comprehensive Cancer Network (NCCN), American Urological Association (AUA), and European Association of Urology (EAU) guidelines, Irreversible Electroporation (IRE/NanoKnife) is generally considered a non-standard, emerging, or investigational option for prostate cancer, particularly as a first-line treatment, largely due to a lack of long-term randomized controlled trial data.
IRE / NanoKnife is considered an emerging technology for treating specific, localized, low-to-intermediate risk tumors.
IRE / NanoKnife should be used in the context of clinical trials or through shared decision-making, acknowledging the limitation of long-term data.
Regulatory Status: While studies exist, some medical policies note that IRE for prostate cancer may still be considered experimental, lacking widespread, long-term, comparative evidence to standard care
Key Takeaways on NanoKnife (IRE) in 2026
Not Yet First-Line: While safe and potentially highly effective (e.g., 97% eradication of the index lesion in some studies), it is not the first-line, standard recommendation for most patients.
Focal Therapy Focus: It is used primarily for focal, or “salvage” (secondary), treatment rather than whole-gland ablation.
Best for Selected Cases: It is typically reserved for men with low-to-intermediate risk prostate cancer who are prioritised for quality of life (e.g., preserving sexual/urinary function).
CONCLUSIONS – VERDICT IN 2026:
More than 50,000 to 100,000 men have been treated globally around the world have with high intensity focused ultrasound for prostate cancer which is the leading clinical application of the focal therapy technology – in fact, more than 50% of all HIFU procedures performed to date around the globe have been for prostatic diseases. The technology has been used to treat a wide variety of prostate-related diagnoses, including benign prostatic hyperplasia (BPH), partial gland cancer, localised whole-gland prostate cancer, and recurrent prostate cancer.
Even with this huge number of cases, there is still absence of actual high qualitative comparative data of HIFU against the standard of care in prostate cancer treatment.
The same goes with all other focal therapy modality treatment in prostate cancer.
With this, all the modalities of focal therapy in prostate cancer, as of 2026, is still considered investigational or experimental, and should only be offered in a well-designed prospective trial setting and be performed within the context of a prospective registry, and after an informed decision.
As of 2024, the American Cancer Society has stated: (https://www.cancer.org/cancer/types/prostate-cancer/treating/cryosurgery.html):
1. It is not yet clear if focal treatments in prostate cancer work as well in the long term (although if the cancer does come back, these treatments can often be repeated, or other treatments can be tried)
2. Most expert groups do not recommend focal ablative therapies as the first line treatment for prostate cancer, unless surgery and radiation aren’t good options. This is mainly because there isn’t enough long-term data to show that these treatments are as effective as surgery or radiation.
HIFU in Malaysia is generally approved for patients meeting the following clinical criteria:
First and foremost: It must be conducted within a prospective registry data collection, at a designated site by a certified / trained urologist, and patients must be informed that it is a non-standard investigational option currently undergoing clinical trials.
1. Disease Stage and Risk
- Localized Prostate Cancer: The cancer must be confined to the prostate gland (Stage T1–T2, N0, and M0).
- Low to Intermediate Risk: The treatment is applicable for Gleason Score 6 (3+3) to 7 (3+4 or 4+3), and in some scenarios, low-volume Gleason 8 (4+4).
- Optimal PSA Levels: Prostate-specific antigen (PSA) levels should typically be below 15 ng/ml, or in some focal protocols, < 20 ng/ml.
- Maximum Involvement: Ideally, less than 50% of prostate biopsies should show cancer involvement.
2. Anatomical and Diagnostic Criteria
- Visible Lesion: A targetable lesion must be visible on multiparametric MRI (mpMRI) or fusion imaging.
- Prostate Size: Prostate volume should generally be less than 40cc to 50cc to ensure effective treatment reach.
- Minimal Calcification: Minimal prostate calcification (measured on TRUS) is required to prevent interference with ultrasound waves.
- No Active Infection: Patients must not have active urinary tract infections.
3. Eligible Patient Profile
- Patients who are not candidates for or choose not to undergo active surveillance.
- Patients who prioritize the preservation of sexual function and urinary control over radical surgery or radiation.
- Patients with localized recurrence after primary radiotherapy (known as salvage HIFU).
4. Approved Facilities and Technology
- The procedure is offered at specialized institutions.
- The procedure uses advanced imaging platforms, to ensure precise, robotically guided targeting.