Radiotherapy is a standard, highly effective treatment for prostate cancer, often offering cure rates comparable to surgery. It is used as a primary treatment for localised disease, combined with hormone therapy for advanced cases, or as salvage therapy after surgery, using precise methods like IMRT, SBRT, or brachytherapy to target cells while sparing healthy tissue.

Linear Accelerator (LINAC) for delivering EBRT
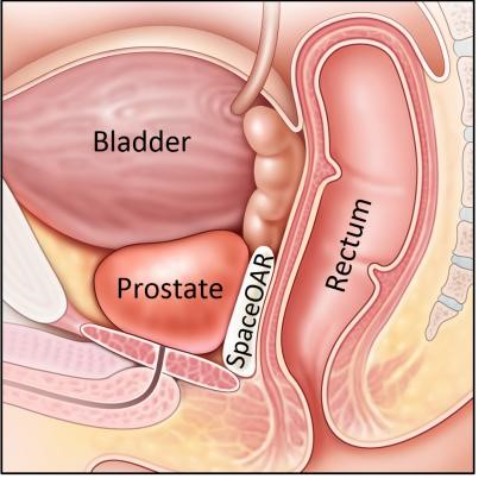
SpaceOAR spacer gel and stereotactic ablative radiotherapy (SBRT) to spare nerve bundles and arteries near the prostate
Advances In Radiotherapy For Prostate Cancer
Radiotherapy advances have manifest in two major, co-related, developments:
More targeted delivery of radiotherapy and dose escalation.
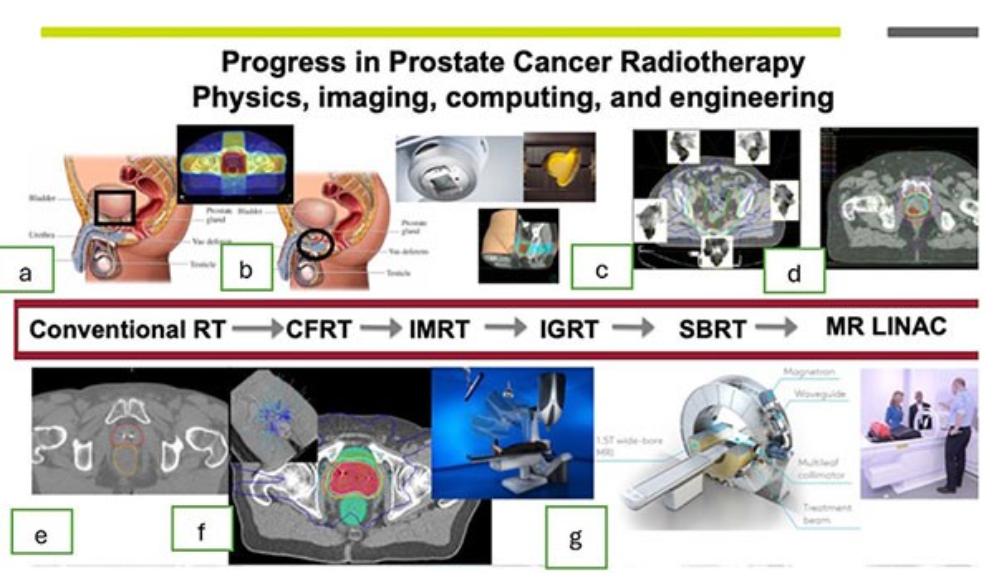
- More targeted radiotherapy delivery, using approaches beginning with conformal radiotherapy (CRT) and evolving to intensity modulated radiotherapy (IMRT) and image guided radiotherapy (IGRT), allows the sparing of adjacent organs (reducing toxicity) while facilitating increase dose delivery to the prostate.
- In addition, facilitating dose escalation, advances in radiotherapy technology have allowed for hypofractionation in which fewer, larger doses of radiotherapy are administered.
Classically, external beam radiotherapy has been administered in a non-fractionated schedule of 1.8 – 2.0 Gy per day, five days per week for 6 to 8 weeks.
However, prostate cancer cells are known to have a higher sensitivity to fractional radiation doses and thus, theoretically, should benefit from hypofractionated schedules. This characteristic is reflected by a low alpha/beta (α/β) value, which is a measure of fractionation sensitivity and is related to the inherent ability of tumor cells to repair sublethal DNA damage inflicted by ionising radiation.
This low alpha / beta (α/β) ratio characteristic of prostate cancer is further accentuated by the high alpha / beta (α/β) ratios of the surrounding tissues, with ratios of 5.6 Gy and 3 Gy estimated for late toxicity effects on the bladder and rectum.
1. Modern Techniques And Precision
IMRT and VMAT: Intensity-Modulated Radiation Therapy (IMRT) and Volumetric Modulated Arc Therapy (VMAT) are the current standards, allowing for complex, sculpted radiation doses that conform to the prostate shape while shielding nearby critical organs, such as the rectum.
IGRT (Image-Guided Radiotherapy): Uses daily image guidance (e.g., using Cone-Beam CT or gold fiducial markers) is crucial. It ensures high treatment accuracy by locating the prostate, which can shift in position, and allows for smaller safety margins, minimising toxicity.
SBRT (Stereotactic Body Radiotherapy): A specialized form of ultra-high-precision radiation (often with CyberKnife or VMAT) that delivers high doses in only 5 fractions, rather than the traditional 19-37+ sessions, providing similar control and fewer late GU side effects.
MR-Linac: Combines MRI with a linear accelerator for real-time imaging during treatment, allowing for adaptive planning to account for daily prostate movement.
2. Treatment Strategy (Fractionation And Boosting)
Hypofractionation (HFRT): Prostate cancer cells have a low alpha / beta ratio (1.5-3.0 Gy), meaning they are more sensitive to larger, fewer doses of radiation compared to surrounding tissues. HFRT, such as 60 Gy in 20 fractions, is considered standard of care.
Ultra-hypofractionation (UHRT): Highly efficient UHRT schedules, like 36.25 Gy in 5 fractions, have shown similar tumour control (95.8% freedom from biochemical failure) in PACE-B trials.
Intraprostatic Boost: Targeting the specific dominant lesion within the prostate (identified by multiparametric MRI) with a higher boost dose improves biochemical disease-free survival.
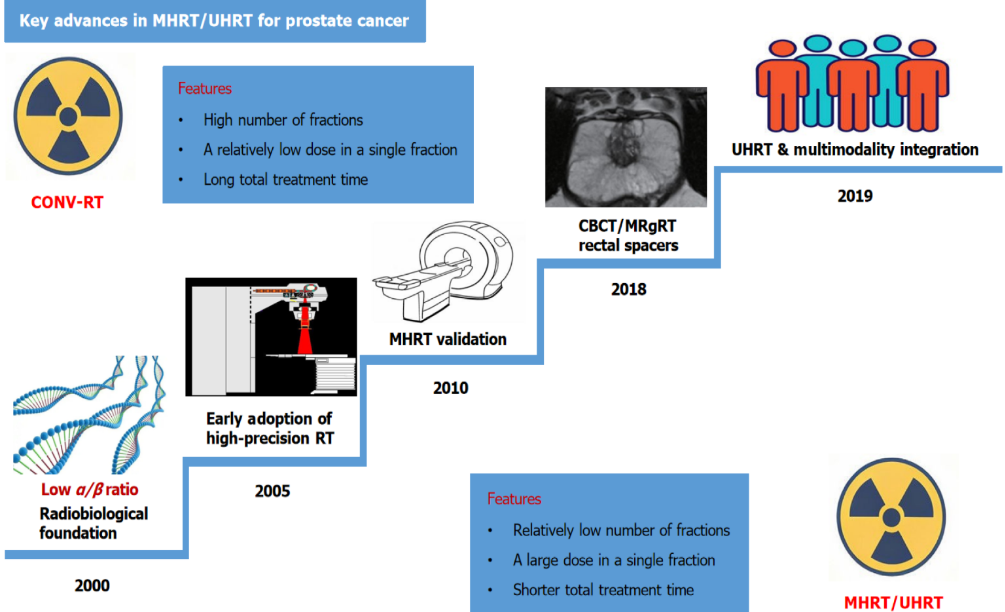
Moderate hypofractionation vs ultra-hypofractionation in prostate cancer
Moderate hypofractionation (MHRT) is generally used as a standard, convenient alternative to conventional therapy (4–6 weeks) for low-to-intermediate risk prostate cancer. Ultra-hypofractionation (UHRT) is used for similar, lower-risk patients desiring maximum convenience (1–2 weeks), particularly when high-precision SBRT is available.
Comparison
Both methods are supported for localised prostate cancer by ASTRO guidelines (often with image-guided IMRT). UHRT provides the best convenience, while MHRT offers a balance of reduced time and extensive clinical data.
Moderate hypofractionation is the “preferred” approach for patients across nearly all risk groups according to the recent NCCN clinical practice guidelines in oncology while ultra-hypofractionation (SBRT) is considered an appropriate regime in most settings apart from regional N1 disease.
3. Combination Therapy (Hormonal Support)
Androgen Deprivation Therapy (ADT): Radiotherapy is more effective when combined with hormonal therapy, which works by reducing testosterone to curb cancer cell growth.
Duration: EAU Guidelines recommend 4-6 months of ADT for intermediate-risk and 24-36 months for high-risk disease in combination with radiotherapy.
4. Side Effects And Management
Acute vs. Late: Side effects can be immediate (early) or long-term (late).
GU/GI Toxicity: Common toxicities affect the bladder (genitourinary – GU) and rectum (gastrointestinal – GI). Modern IMRT/IGRT has significantly reduced these.
Secondary Cancers: There is a slight, rare risk (1 in 70 patients surviving >10 years) of developing secondary cancers in the bladder or rectum after external radiation, though this is not typically seen with brachytherapy.
5. Other Treatment Settings
Post-prostatectomy Setting:
Adjuvant radiotherapy (ART) is used immediately after surgery if risk factors are present, while Salvage Radiotherapy (SRT) is used if PSA rises later.
The RADICALS-RT trial suggested that saving RT for the salvage setting can reduce unnecessary toxicity, although SRT may be better suited for high-risk patients.
Long-term results from RADICALS-RT trial confirm adjuvant RT after radical prostatectomy increases the risk of urinary and bowel morbidity, but does not meaningfully improve disease control. An observation policy with salvage RT for PSA failure should be the current standard after radical prostatectomy.
RADICALS-RT results support the use of early salvage radiotherapy for PSA failure after radical prostatectomy rather than early adjuvant intervention
Metastatic Disease:
Radiotherapy to the primary tumour in low-volume metastatic disease – as proven in the STAMPEDE (Arm H) and HORRAD trials – can provide a survival advantage.
6. Clinical Evidence Base
Key Trials: CHHiP (hypofractionation), PACE (SBRT), FLAME (boost), and HYPO-RT-PC (ultra-hypofractionation) provide the randomised evidence for modern standards.
Quality of Life: The ProtecT trial indicated that 15-year survival rates are similar between radical prostatectomy, radiotherapy, and active monitoring, making treatment decisions heavily reliant on personal preferences regarding side-effect profiles (e.g., urinary vs. bowel issues).
ADT Duration With EBRT
For prostate cancer treated with external beam radiotherapy (EBRT), the duration of androgen deprivation therapy (ADT) depends primarily on the risk classification of the cancer.
High-Risk Prostate Cancer: Long-term ADT is typically recommended. Studies suggest that for patients receiving EBRT alone (without a brachytherapy boost), a duration of 18 months or more is beneficial, with some findings suggesting a longer duration (e.g., 28 months) may be more effective than a shorter one (e.g., 18 months).
Intermediate-Risk Prostate Cancer: Short-term ADT is the standard of care, with the duration often lasting several months, usually 6 months.
Low-Risk Prostate Cancer: ADT is generally not recommended as it provides no survival benefit.
Key Considerations And Modifications:
With Brachytherapy Boost: If a brachytherapy boost is used in addition to EBRT, a shorter duration of ADT may be sufficient for high-risk patients.
Timing: ADT often commences prior to the start of radiation, as this overlap maximizes synergy.
Response-Based Adjustment: In high-risk patients, the total duration may be adjusted based on treatment response; for instance, achieving a very low nadir PSA may allow for a shorter duration of ADT, while those not reaching this level may require a longer duration
Prostate-Only Radiation Therapy vs Whole-Pelvis Radiotherapy (PO-RT VS WP-RT)
External beam radiotherapy (EBRT) for prostate cancer can be delivered either as Prostate-Only Radiation Therapy (PORT), targeting just the prostate gland, or as Whole-Pelvis Radiotherapy (WPRT), which includes the prostate and nearby pelvic lymph nodes.

Evidence suggests that whole pelvic radiotherapy (WPRT) for high-risk prostate cancer significantly improves biochemical recurrence-free survival (BRFS) and distant metastasis-free survival (DMFS) compared to prostate-only radiation therapy (PORT), but it generally does not show a significant improvement in overall survival (OS).
Toxicity: WPRT is associated with higher acute gastrointestinal (GI) and genitourinary (GU) toxicity compared to PORT.
WPRT Benefits High-Risk Patients: Studies suggest WPRT is superior to PORT in reducing biochemical recurrence (PSA rise) in high-risk and very-high-risk patients, often combined with ADT (Androgen Deprivation Therapy).
Toxicity Trade-off: WPRT generally increases the risk of acute (short-term) gastrointestinal (GI) and genitourinary (GU) side effects compared to PORT.
Similar Survival: Most studies show no significant difference in overall survival between WPRT and PORT, despite improvements in disease-free survival with WPRT.
Comparison: PORT vs. WPRT
| Feature | PORT (Prostate Only) | WPRT (Whole Pelvis) |
| Target Area | Prostate gland (± seminal vesicles) | Prostate + Pelvic Lymph Nodes |
| Primary Use | Low/Intermediate-risk disease | High/Very-high-risk disease |
| Recurrence Risk | Higher risk of nodal recurrence | Lower risk of nodal recurrence |
| 5-yr PSA Control | Generally lower (77-81%) | Higher (84-95% in high-risk) |
| Toxicity | Lower GI/GU side effects | Higher acute GI/GU side effects |
Best Patient Candidates: WPRT is most beneficial for high-risk or very-high-risk patients, particularly those with an estimated pelvic nodal risk >20% (Roach formula) or those receiving high-dose-rate (HDR) brachytherapy boost.
Summary Table of Comparative Data (High-Risk/Very High Risk)
| Outcome (5-year) | WPRT | PORT |
| BRFS (Biochemical recurrence free survival | Higher (e.g., 95%) | Lower (e.g., 81.2%) |
| DMFS (Distant metastasis-free survival) | Better (e.g., 95.9%) | Lower (e.g., 89.2%) |
| Overall Survival | Similar (No Sig. Diff) | Similar (No Sig. Diff) |
| Acute Toxicity | Higher | Lower |
Conclusion
For high-risk prostate cancer, adding pelvic radiation to the prostate treatment (WPRT) provides superior biochemical control and a lower risk of metastasis, making it a valuable option for managing micrometastatic disease, even if a direct, long-term overall survival benefit is not statistically proven in all studies.
Current Role, Indication, Efficacy And Significance Of Proton Beam Therapy Or Particle Beam Therapy In Prostate Cancer
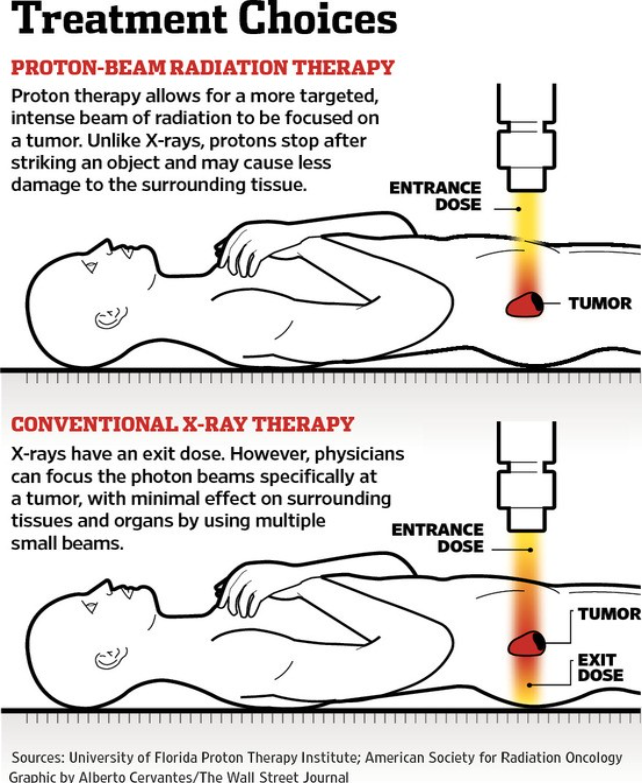
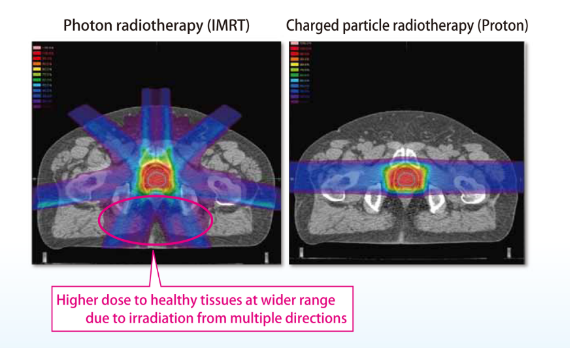
Conventional EBRT uses high-energy X-rays (photons) that enter the body, pass through the tumor, and exit the body, exposing surrounding healthy tissue to radiation.
In comparison, Proton Beam Therapy uses positively charged proton particles that accelerate to a specific depth, stop at the tumor, and release the majority of their energy directly into the cancer, causing significantly lower doses to nearby organs at risk.
As of 2026, Proton Beam Therapy (PBT) and other Particle Beam Therapies (such as Carbon Ion Therapy and Boron Neutron Capture Therapy / BNCT) represent the “precision frontier” of external radiation. While their biological effectiveness is similar to advanced X-ray techniques, their significance lies in the physics of how they deliver energy.
1. The Core Role: The “Bragg Peak” Advantage
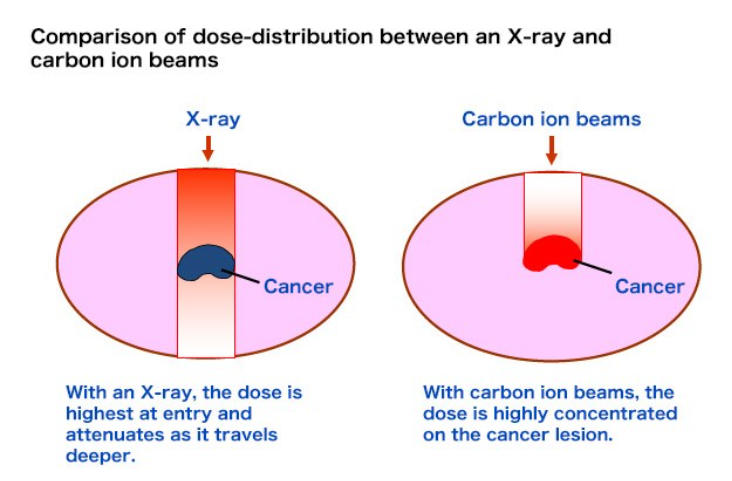
The primary role of PBT is to exploit a physical phenomenon called the Bragg Peak.
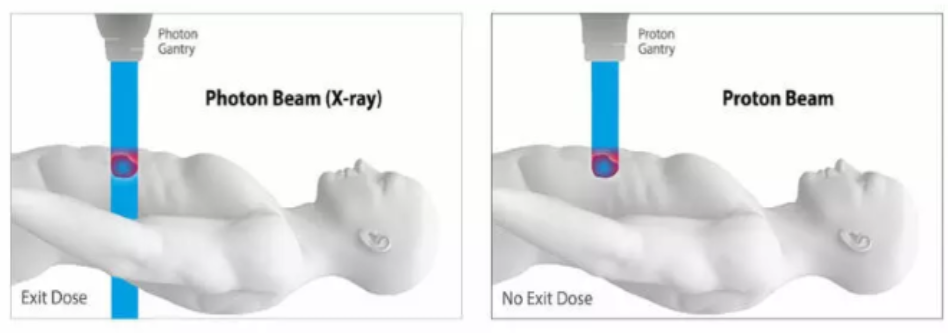
- The Physics: Unlike standard X-rays (photons) which pass all the way through the body, protons are heavy charged particles that travel to a specific depth and then stop. They deposit the bulk of their energy at the very end of their path.
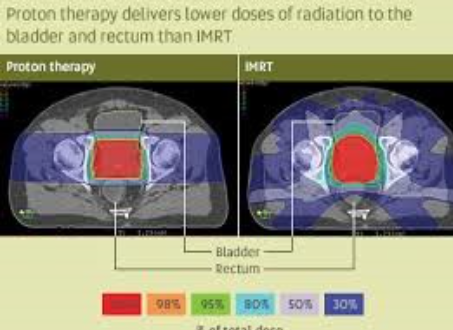
- The Result: This virtually eliminates the “exit dose.” The tissue behind the prostate receives almost zero radiation, theoretically sparing the anterior wall of the rectum and the bladder more effectively than standard IMRT.
Current Indications (2026)
While PBT can be used for any localised prostate cancer, it is most specifically indicated in these scenarios:
- High-Risk / Nodal Disease: For patients requiring pelvic lymph node irradiation. PBT’s precision helps limit the “integral dose” (total radiation absorbed by the body), reducing the risk of secondary cancers and bowel toxicity in these larger treatment fields.
- Recurrent Disease (Re-irradiation): If a patient has already had radiation and the cancer returns, PBT is often the preferred choice because it can target the recurrence while strictly avoiding nearby organs that have already reached their lifetime radiation limit.
- Younger Patients: Due to the lower integral dose, PBT is indicated for younger men to minimize the long-term risk of radiation-induced secondary malignancies.
3. Efficacy & Clinical Significance
The debate in 2026 focuses on whether “better physics” equals “better clinical outcomes.”
- Efficacy: Large-scale data (including updates from registries and prospective trials) show that PBT is as effective as IMRT in curing prostate cancer. PSA control and survival rates are essentially identical.
- Toxicity/Side Effects: Research remains mixed. While dosimetric studies show PBT spares more healthy tissue, clinical trials have not consistently proven a massive reduction in side effects compared to the most advanced X-ray techniques (VMAT/IMRT).
- Modern Evolution (2026): The launch of “Proton-SBRT” (Ultrahypofractionation) is a significant 2026 milestone. Centers are now delivering PBT in just 5 fractions over two weeks, matching the convenience of X-ray SBRT while maintaining proton precision.
4. Other Particle Beam Therapies (Carbon Ion)
Beyond protons, Carbon Ion Radiotherapy (CIRT) is gaining research traction, particularly in specialized centers in Japan and Europe.
- Significance: Carbon ions are even heavier than protons. They have a lower Alpha/Beta ratio sensitivity and a higher Relative Biological Effectiveness (RBE).
- The Role: CIRT is being investigated for “radioresistant” prostate cancers (those that don’t respond well to standard radiation) because the carbon ions cause more complex, lethal DNA damage that the cancer cells cannot repair.
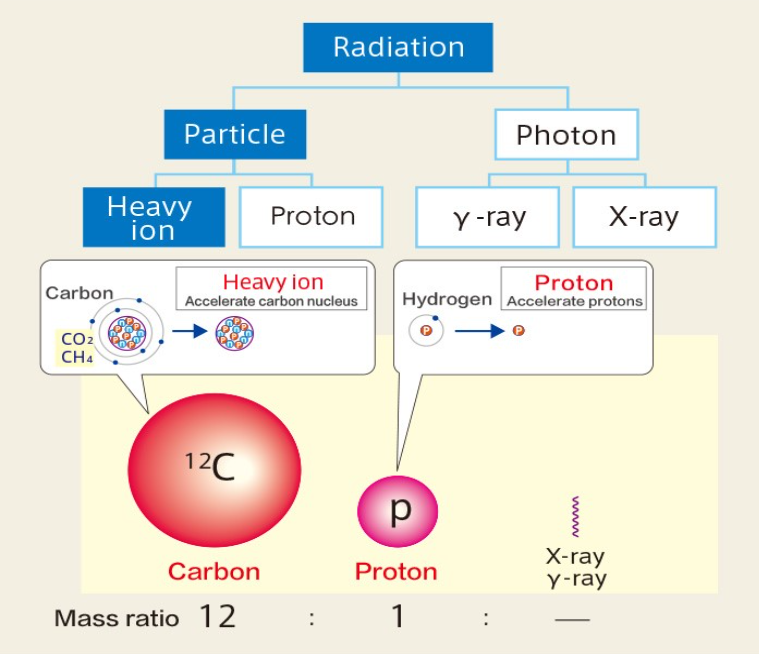
Therapeutic radiation is categorised into either a photon beam, or a particle beam. A photon beam is a kind of electromagnetic wave, and a particle beam is made up of high-energy ions. The former includes X-rays and gamma rays, and the latter includes protons and heavy ions
5. Summary of Treatment & Dosages (2026)
| Modality | Typical Dose/Fractions | Total Dose | Significance |
| PBT (Standard) | 1.8–2.0 GyE x 38–40 | 70–80 GyE | High precision; standard for decades. |
| PBT (Hypo) | 2.5–3.0 GyE x 20 | 60 GyE | Current efficient standard. |
| PBT (SBRT) | 7.5–8.0 GyE x 5 | 37.5–40 GyE | The 2026 standard for convenience. |
Summary of Treatment Indications
| Modality | Risk Group | Typical Schedule | Duration |
| Conventional EBRT | Any | 1.8 Gy x 40–45 | 8–9 Weeks |
| Moderate Hypo | Low / Intermediate | 3.0 Gy x 20 | 4 Weeks |
| SBRT (Ultra-Hypo) | Low / Intermediate | 7.5 Gy x 5 | 1–2 Weeks |
| HDR Boost + EBRT | High Risk / Locally Adv. | EBRT (5 weeks) + 15 Gy HDR | 6 Weeks Total |
| Palliative RT | Metastatic (Bone pain) | 8 Gy x 1 or 4 Gy x 5 | 1 Day to 1 Week |
Strategic Note: For a patient in Malaysia, Proton Beam / Particle Beam Therapy is a highly specialised “niche” modality. While it offers superior “dosimetric” maps (the pictures look better), a senior experienced oncologist would typically weigh the significantly higher cost against the fact that modern X-ray IMRT (with a hydrogel spacer) achieves very similar real-world safety profiles. The choice often comes down to the patient’s age, anatomy, and specific risk of secondary cancers.
Key 2026 Trends:
SBRT And Hypofractionation:
Stereotactic Body Radiotherapy (SBRT) is increasingly established as a safe, effective, and efficient standard of care, offering high-level cancer control while limiting side effects. Recent studies have validated extreme hypofractionation (fewer, higher-dose fractions) against traditional treatments.
Stereotactic Body Radiation Therapy (SBRT) is now considered a standard of care for localized low- and intermediate-risk prostate cancer.
Recent clinical trials (such as PACE-B) have demonstrated that SBRT is non-inferior to conventional External Beam Radiation Therapy (EBRT) in terms of cancer control and toxicity.
Key Comparisons
| Feature | Conventional EBRT | SBRT (Ultrahypofractionation) |
| Treatment Duration | 4 to 8 weeks | 1 to 2 weeks |
| Number of Sessions | 20 to 44 fractions | 5 fractions |
| Precision | High | Ultra-high (Sub-millimeter) |
| Effectiveness | ~95% success at 5 years | ~95% success at 5 years |
Why the Shift?
- Convenience: SBRT reduces the number of hospital visits significantly.
- Radiobiology: The prostate may be more sensitive to larger doses of radiation per fraction (high α/β ratio), making SBRT theoretically more effective.
- Safety: Modern image-guided technology allows for tight margins, sparing the bladder and rectum similarly to traditional methods.
Note: For high-risk cases, SBRT is still being evaluated and is often used as a “boost” alongside conventional EBRT rather than a standalone treatment.
Post-surgery Radiotherapy:
The POSEIDON meta-analysis is a landmark study published in The Lancet and presented at the 2026 ASCO Genitourinary Cancers Symposium which pooled individual patient data from 6,057 participants across six phase 3 trials to evaluate the benefit of adding hormone therapy (HT) to postoperative radiotherapy for recurrent prostate cancer.
Data from the 2026 POSEIDON (Post-Operative Salvage or Adjuvant Radiotherapy and anti-androgen therapy for men with prostate cancer) meta-analysis suggests that adding short – or long-term hormone therapy to salvage radiotherapy provides no survival benefit for most men, particularly those with a pre-radiation PSA level below 0.5 ng/mL.
Hormone therapy is now recommended mainly for those with higher PSA levels (>0.5 ng/mL).
- The POSEIDON study, a meta-analysis of individual patient data from six phase III randomized trials, examined whether patients with prostate cancer benefit from the addition of hormone therapy to post-prostatectomy radiotherapy.
- The addition of hormone therapy did not improve survival in the overall patient population.
- However, there was an improvement in overall survival for patients with a prostate-specific antigen (PSA) level above 0.5 ng/mL at the time of radiation therapy. Survival benefits only began to emerge significantly when pre-PORT PSA levels exceeded 0.5 ng/mL, with the greatest benefit seen in patients with very high levels above 1.6–2.0 ng/mL
- There was no added benefit with prolonged hormone therapy (24 months); this suggests short-term therapy (4–6 months) is adequate in this clinical setting.
Radiotherapy In Metastatic Disease:
Local prostate radiotherapy (e.g., to the primary tumor) is recommended to improve survival in patients with low-volume metastatic castration-sensitive prostate cancer (mCSPC) and can delay local complications.
Evidence of this primarily came from the STAMPEDE trial (Trial Arm H / Radiotherapy arm), demonstrating that adding radiotherapy (RT) to the prostate in patients with newly diagnosed, low-volume (oligometastatic) disease significantly improves overall survival, specifically in patients receiving androgen deprivation therapy (ADT); providing a 32% survival improvement and delays the onset of castration resistance.
A separate, newer trial STAMPEDE 2 is now testing SBRT (comparison S arm) to 177Lu-PSMA-617 (comparison P arm) to treat oligometastatic sites and whether this can further improve survival and quality of life.
Particle Beam Therapy:
Due to a lack of direct evidence, the superiority of particle beam RT over conventional photon beam RT or other particle beam therapies for prostate cancer has not been confirmed in terms of the rates of overall survival or bRFS (biochemical relapse‐free survival) as end‐points.
However, charged particles, such as protons and carbon ions, reduce the irradiated volumes and doses in the organs at risk surrounding the prostate, and previous studies have shown very low incidences of GI and GU toxicities after particle beam RT.
Long‐term observation in a large‐scale randomised study is necessary for the most accurate evaluation of the efficacy of particle beam RT for prostate cancer, but particle beam RT seems a reasonable RT method delivering a high RT dose safely.
As of early 2026, the verdict on particle beam therapy – specifically Proton Beam Therapy (PBT) and Carbon Ion Radiotherapy (CIRT) – for prostate cancer is that it is a safe, highly effective, and dosimetrically superior treatment. However, its role in standard clinical practice is characterised as an advanced, specialized option rather than a necessary replacement for modern photon therapy (IMRT/SBRT), largely because comparative trials have shown similar long-term oncological outcomes.
Clinical Guidance In 2026:
Particle beam therapy is best suited for patients seeking to minimise lower-dose exposure to normal tissues (such as younger patients) or those with challenging anatomy where conventional photon radiotherapy cannot spare surrounding critical structures
Optimal Management Strategies:
Advanced Imaging (PSMA PET): Routine use of advanced imaging is reshaping radiotherapy, allowing for better identification of nodes and targeted boost techniques.
Biomarkers: Genomic classifiers (e.g., Decipher Prostate test – analyzes tumor RNA from biopsies or surgical samples to predict the aggressiveness of prostate cancer) are becoming essential to identify high-risk patients who need intensified therapy.
Radium-223: Continued studies (DORA, PEACE-3) in 2026 confirm its role in treating advanced, bone-metastatic disease in combination with systemic therapies.