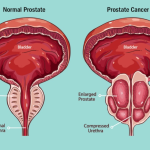
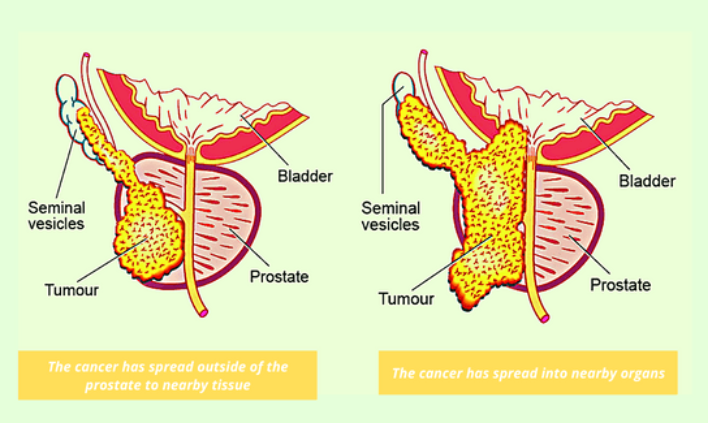
Locally advanced prostate cancer (LAPC) refers to tumors that have grown outside the prostate capsule or spread to immediately adjacent tissues (like the seminal vesicles or pelvic wall) but has not yet metastasised to distant organs.
Management relies on a multimodal approach using radiation therapy, hormonal therapy, and sometimes surgery. While there is no global consensus on the optimal curative approach, three major medical organizations – the European Association of Urology (EAU), the American Urological Association (AUA), and the National Comprehensive Cancer Network (NCCN) – provide evidence-based frameworks.
Management typically relies on a multimodal combination of external beam radiation therapy (EBRT), radical prostatectomy (RP), and androgen deprivation therapy (ADT).
While all three organizations agree that multimodal therapy offers the best outcomes for high-risk patients, their primary guidelines vary slightly in the sequencing and duration of ADT and the preferred role of surgery.
Defining Locally Advanced Prostate Cancer
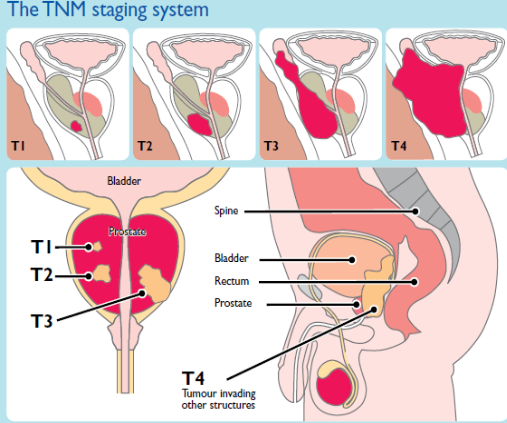
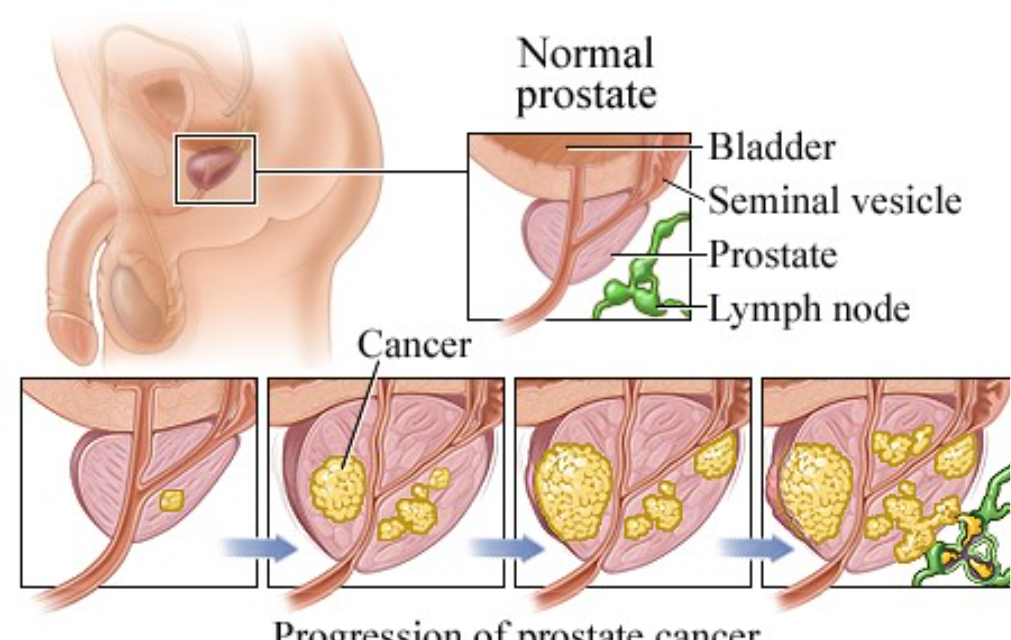
To accurately classify Locally Advanced Prostate Cancer, urologists and oncologists utilize the TNM (Tumor, Node, Metastasis) Staging System and risk grouping criteria from organizations such as the National Comprehensive Cancer Network (NCCN) and the European Society for Medical Oncology (ESMO).
The disease is categorized by the following features:
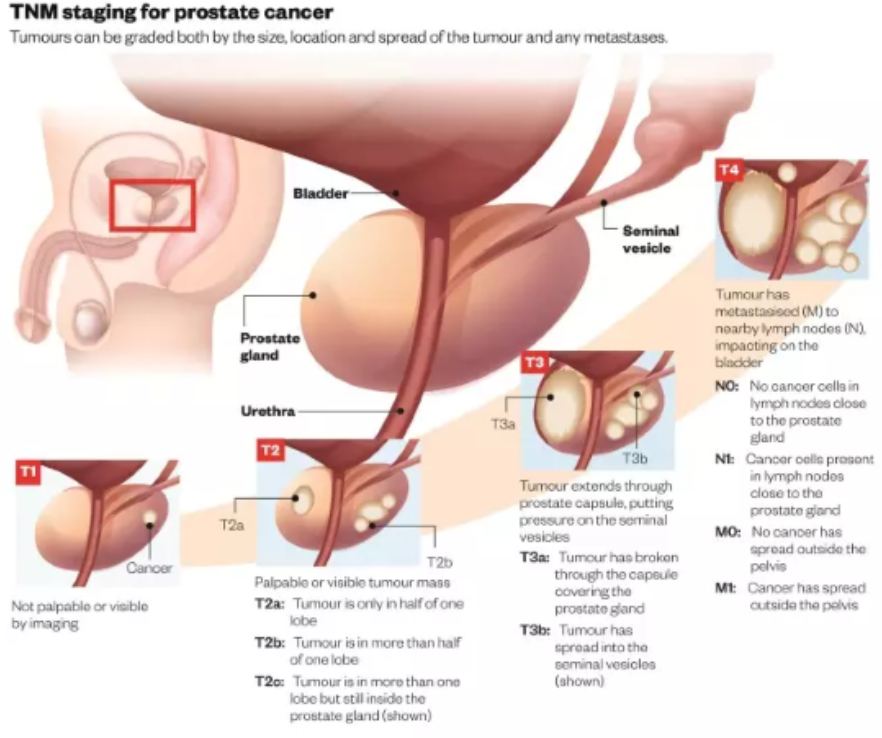
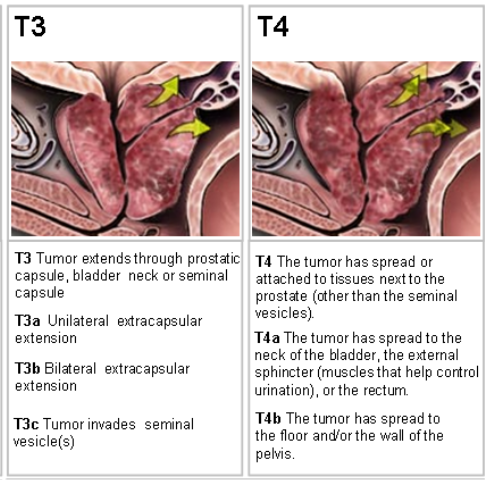
T-Category (Stage T3-T4): Refers to the physical extent of the primary tumor.
T3a: Extracapsular extension (tumor has broken through the outer shell of the prostate).
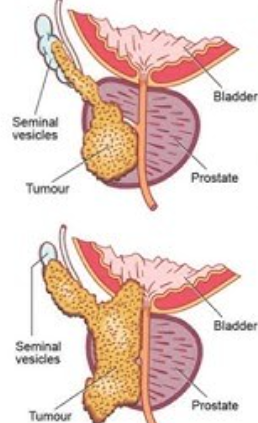
T3b: Tumor has invaded the seminal vesicles.
T4: Tumor has invaded other adjacent structures, such as the bladder neck, rectum, or pelvic wall.
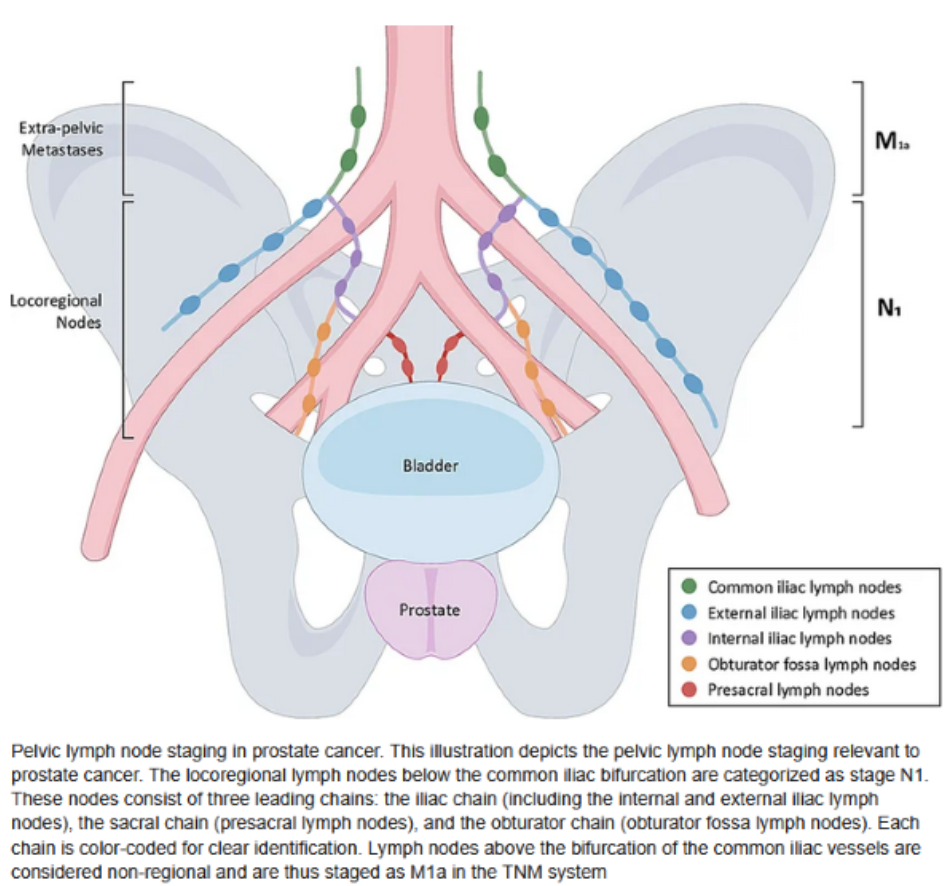
N-Category (Node-Positive, M0): Regional lymph node involvement (N1) is often evaluated alongside T-stage. If the cancer has spread to local lymph nodes but not to distant bones or organs, it is classified as locally advanced.
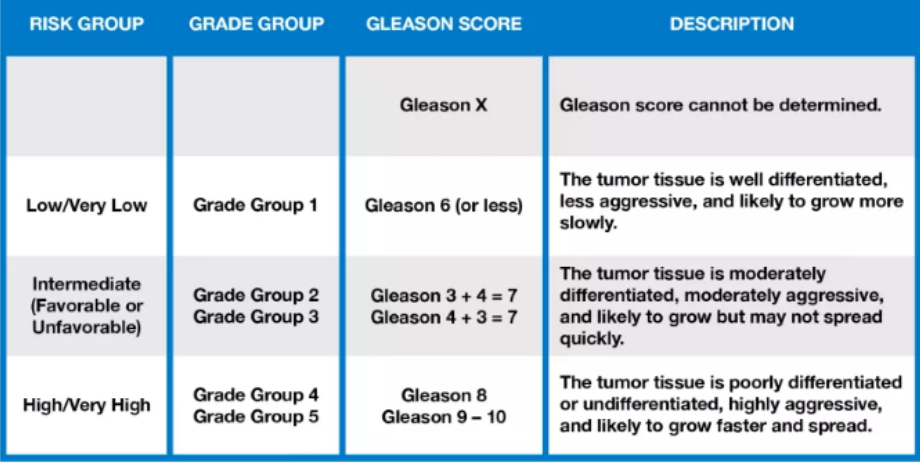
High-Risk Localized (Very High Risk): While this is strictly localized and not locally advanced disease, patients with a Gleason Score of 8–10 or Prostate-Specific Antigen (PSA) levels >20 ng/mL are treated in a manner nearly identical to locally advanced cases because of the high likelihood of subclinical spread.
Comparison of Clinical Guidelines for Locally Advanced Prostate Cancer
| Clinical Pathway | EAU (European Association of Urology) | AUA (American Urological Association) | NCCN (National Comprehensive Cancer Network) |
| Primary Approach for Fit Patients | Multimodal approach. Long-term ADT combined with EBRT is standard. Surgery (RP) + extended pelvic lymph node dissection is reserved for select, resectable cases. | Strong focus on EBRT combined with ADT. RP is an option for very carefully selected clinical T3 patients as part of a multimodal plan. | Multimodal is preferred. Recommends EBRT + ADT. Radical prostatectomy + extended lymph node dissection is a primary option for highly selected patients. |
| Duration of ADT | Recommends long-term ADT (24–36 months) combined with primary radiotherapy for high-risk/locally advanced disease. | Typically recommends EBRT with concurrent and adjuvant ADT (usually 18–36 months). | Recommends EBRT with short-term ADT (4–6 months) for favorable intermediate, or long-term ADT (24–36 months) for high-risk/T3-T4 LAPC. |
| Adjuvant / Salvage Therapy | Adjuvant ADT/RT is evaluated based on post-surgery pathological staging (e.g., positive margins, seminal vesicle invasion). | Salvage RT is recommended for biochemical recurrence. Adjuvant therapy strongly considered for adverse pathology. | Observation, ADT, or salvage RT depending on post-surgical PSA levels and pathological findings. |
| Neoadjuvant ADT | Recommends against the use of neoadjuvant (pre-treatment) ADT prior to radical prostatectomy outside of clinical trials. | Recommends against routine neoadjuvant ADT prior to radical prostatectomy. | Does not generally recommend neoadjuvant ADT for patients undergoing primary radical prostatectomy. |
| Follow-up / Surveillance | Strict PSA monitoring intervals and multiparametric MRI if a recurrence is suspected. | Individualized follow-up strategy with regular PSA and symptom assessment. | Standardized follow-up (PSA every 6-12 months for 5 years, then annually) with targeted imaging based on PSA doubling time. |
Focusing on the management of the various subcategories of locally advanced prostate cancer
Due to its heterogeneity, and paucity of randomized clinical trials on locally advanced prostate cancer, the treatment of locally advanced prostate cancer should include the various subcategories:
1. Treatment of locally advanced, nodal negative disease (T3, N0 disease)
2. Treatment of locally advanced, nodal positive disease (N1 disease)
i. Clinical node positive disease cN1 based on imaging pre-treatment
ii. Post radical prostatectomy with pathological nodal positive disease pN1, categorized into low volume (1-2) and high volume (more than 3 nodes) pelvic regional nodal disease
3. Treatment of locally advanced, nodal negative disease, with rectal infiltration (T4 disease)
4. Treatment of post-radical prostatectomy positive surgical margin (PSM+ve) with nodal negative disease
5. Recurrent prostate cancer including Rising PSA post primary treatment – post radical prostatectomy and post EBRT
Management of Subcategories of Locally Advanced Disease
Locally advanced prostate cancer (LAPC) is not a monolith; it comprises a broad spectrum of clinical presentations. Management is highly individualized based on the patient’s exact subcategory, overall health, and life expectancy. Due to its heterogeneity, and paucity of randomized clinical trials on locally advanced prostate cancer, the treatment should be specifically individualized.
1. Non-Metastatic LAPC (T3-T4, N0, M0)
The standard of care for non-metastatic, locally advanced disease is a combination of External Beam Radiation Therapy (EBRT) and Androgen Deprivation Therapy (ADT).
EBRT + ADT: Studies have overwhelmingly shown that combining radiation with hormonal therapy yields superior survival outcomes compared to either treatment alone.
Treatment Duration: ADT is typically administered for a long duration, generally spanning 28 to 36 months in conjunction with radiation.
Advanced Additions: Clinical trials and modern guidelines—such as the NCCN Guidelines – now also suggest adding novel hormonal agents like abiraterone acetate to the EBRT/ADT regimen for high-risk and very high-risk patient subsets to further reduce recurrence rates.
2. Node-Positive LAPC (Any T, N1, M0)
When the cancer has spread to regional pelvic lymph nodes but not beyond, the disease carries a high risk of systemic failure. Management requires a more aggressive, multi-modality approach.
Primary Systemic Therapy and radiotherapy (RT): The foundation of treatment remains systemic ADT combined with pelvic radiation to address both the primary tumor and the affected lymph nodes.
Surgical Options: In highly selected, very fit patients, Radical Prostatectomy (RP) combined with an extended pelvic lymph node dissection (ePLND) can be a viable first step. Surgery is usually followed by adjuvant (post-operative) radiation and/or hormonal therapy depending on the final pathology.
3. High-Risk / Very High-Risk Localized Disease
Patients with massive primary tumors or very aggressive cell profiles (e.g., Gleason score of 9 or 10 are clinically managed similarly to locally advanced cases because of the high likelihood that microscopic cells have already escaped the prostate.
Multimodal Strategy: Primary treatments include either radical prostatectomy (with lymph node removal) or EBRT combined with long-term ADT.
Genomic and Biomarker Testing: Contemporary guidelines increasingly recommend somatic genomic testing (like the Decipher molecular assay or testing for BRCA mutations) to identify specific targets for therapy and better tailor prognoses.
4. Frail or Elderly Patients
For older patients with a limited life expectancy (less than 10 years) or significant comorbidities, the aggressive toxicity of combined EBRT and long-term ADT may outweigh the benefits.
Hormone Therapy Alone: ADT may be used as a monotherapy to shrink the tumor, prevent urinary obstruction, and provide long-term disease control.
Watchful Waiting: In asymptomatic patients with other life-limiting conditions, a watchful waiting (observation) approach may be adopted, delaying hormone therapy until the patient becomes symptomatic.
Contemporary management of locally advanced prostate cancer with various subcategories
Contemporary management of locally advanced prostate cancer requires highly individualized multimodal approaches tailored to the specific pathological findings. Treatment often integrates Androgen Deprivation Therapy (ADT), External Beam Radiation Therapy (EBRT), novel systemic therapies, and surgery.
| Subcategory | Contemporary Management Strategy |
| Positive Surgical Margin (PSM) Post-Radical Prostatectomy | Observation (Early Salvage RT): Preferred if PSA is undetectable, closely monitored with frequent Prostate-Specific Antigen (PSA) tests. Adjuvant Radiation Therapy (ART): Historically recommended for high-risk PSM, though modern management leans toward early salvage radiation (SRT) before PSA rises above 0.2 ng/mL. Consider ADT: May be combined with salvage EBRT depending on initial Gleason score and margin extent. |
| Seminal Vesicle Invasion (SVI) | Multimodal Standard: Typically treated with EBRT combined with long-term ADT (usually 2-3 years for intensification, plus pelvic radiation). Post-Surgery (pT3b): If found on pathology post-radical prostatectomy, treatment is adjuvant EBRT + ADT. |
| Lymph Node Positive Disease (N1) | Definitive/Primary Setting: Standard of care is EBRT with long-term ADT (preferred 2-3 years). Treatment Intensification: For high-risk N1 disease, intensification with novel anti-androgens (e.g., abiraterone) is recommended. Post-Surgery: Management involves pelvic nodal radiation + ADT, sometimes utilizing extended pelvic lymph node dissection. |
| Rectal Infiltration | Advanced Local Therapy: Considered a locally advanced or T4 stage tumor. Standard of care is typically primary definitive EBRT combined with long-term ADT. Multidisciplinary Tumor Board Review: Radical surgery alone is rarely curative and often technically SVI and rectal wall-bound, necessitating neoadjuvant ADT and/or chemotherapy, or pelvic exenteration in highly specialized centers. |
Management plans require guidance from multidisciplinary reviews and genomic/biomarker evaluations where appropriate
The Role of Radical Prostatectomy in Locally Advanced Prostate Cancer
Historically, surgery was rarely recommended for locally advanced disease due to the difficulty of completely clearing the tumor. However, modern surgical techniques, including robotic-assisted laparoscopic prostatectomy, have increasingly made surgery a viable primary option for highly selected T3/T4 patients. Surgery provides precise pathological staging and can be an effective component of a broader multimodal treatment plan, often followed by radiation or hormonal therapy if high-risk features are identified in the surgical pathology.
Nuances in Decision Making
While the table highlights high-level consensus, individual patient factors heavily influence treatment selection. The integration of modern imaging, such as PSMA-PET/CT, is now heavily emphasized across all three guidelines to rule out low-volume metastatic disease before committing to a purely local or locally advanced treatment strategy.
Furthermore, NCCN guidelines heavily emphasize the use of germline/somatic genetic testing (such as looking for BRCA1/BRCA2 mutations) in high-risk populations, as this information may guide future treatment decisions and assess family risk. EAU and AUA lean heavily into performance status and patient life expectancy, generally advocating for active treatments in men with a life expectancy greater than 10 years.
Summary of Future Directions and Considerations
Managing Locally Advanced Prostate Cancer hinges heavily on highly coordinated care between urologists and radiation oncologists. Modern diagnostics, such as PSMA PET scans, have vastly improved the ability of physicians to rule out distant metastases, ensuring that patients are properly classified as locally advanced rather than metastatic.
The integration of genomic testing and next-generation anti-androgen therapies continues to shape personalized, patient-centric treatment plans.
Verdict in 2026
What is the current verdict in 2026 on the contemporary management of locally advanced prostate cancer?
In 2026, the consensus for managing locally advanced prostate cancer (Stage III) centers on highly personalized, multimodal therapy. The standard approach combines external beam radiation therapy (EBRT) with long-term androgen deprivation therapy (ADT), increasingly supplemented by next-generation agents to improve overall survival.
The contemporary verdict and best practices in management include:
- Multimodal Therapy: The gold standard is a combination of long-term ADT and EBRT. Recent guideline updates emphasize treatment intensification, such as adding agents like abiraterone to the standard ADT/RT mix to improve survival outcomes in high-risk patients.
- Targeted Imaging and Staging: Advanced imaging—specifically PSMA PET—has become the standard of care to accurately stage patients and rule out hidden metastasis before committing to a local curative treatment plan.
- Genomic Profiling: Biomarker and genomic testing (e.g., Decipher tests) are routinely utilized to analyze tumor aggressiveness. This tailors the duration of ADT (typically 12 to 36 months) to the individual rather than applying a blanket recommendation.
- Radical Prostatectomy (RP): While EBRT is often preferred, RP with extensive pelvic lymph node dissection is reserved for carefully selected cases, usually as part of a multimodal plan (e.g., surgery followed by adjuvant radiation).
- Focus on Quality of Life: De-escalation and intermittent ADT strategies are actively being explored to mitigate the long-term toxicity (e.g., sexual dysfunction, fatigue, and bone loss) associated with hormone therapies without compromising cancer control