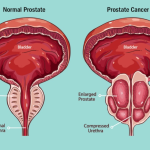
Localised prostate cancer refers to cancer strictly contained within the prostate gland, having not spread to the capsule, surrounding tissues, or distant parts of the body. It is often described as “organ-confined” or “early-stage” prostate cancer. This corresponds to clinical T1 or T2 stages, meaning the cancer has not spread beyond the prostatic capsule.
Treatment options for localised prostate cancer include active surveillance, surgery, or radiation, with high survival rates.
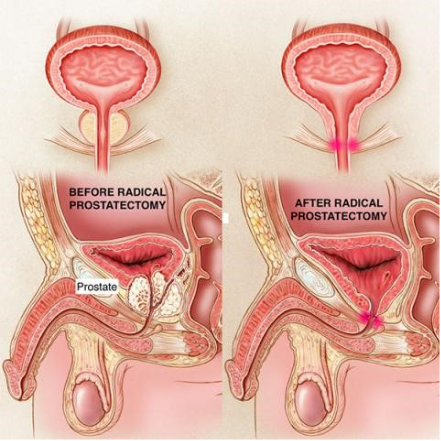
Radical prostatectomy approaches
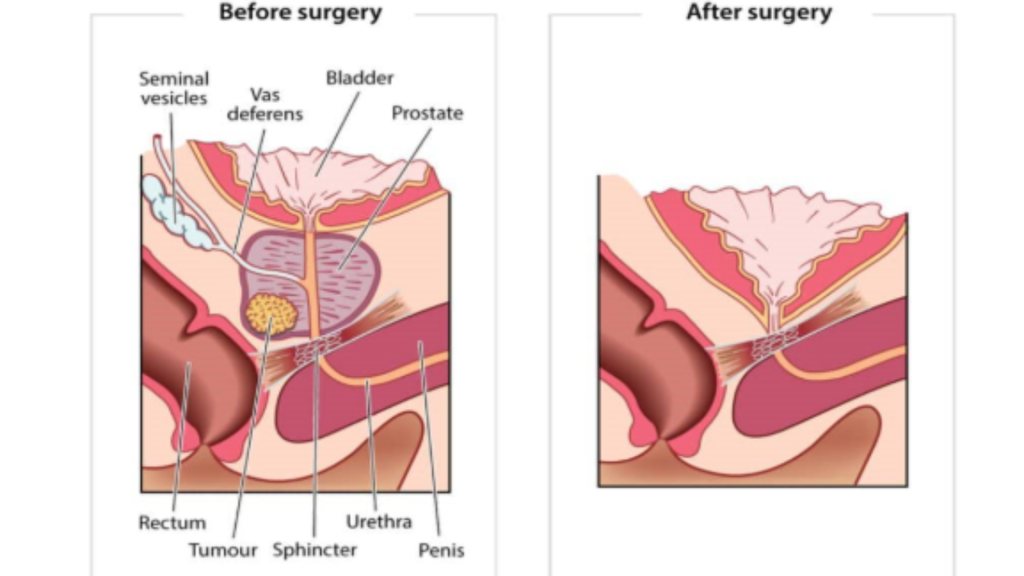
Surgery in prostate cancer (called Radical Prostatectomy; consisting of removal of the whole prostate with the seminal vesicles and sometimes nearby lymph nodes. The bladder is then reattached directly to the urethra) involves various approaches.
The various approaches include open retropubic radical prostatectomy (via an incision on the lower abdomen), radical perineal prostatectomy (via an incision on the perineum – the region between the genitals and the anus, situated between the thighs), laparoscopic radical prostatectomy (by keyhole incisions on the abdomen) and robotic assisted radical prostatectomy (by using a computer assisted surgery via similar keyhole incisions on the abdomen). The incisions made by laparoscopic and robotic radical prostatectomy is exactly the same except the latter uses a computer to assist in the surgery.
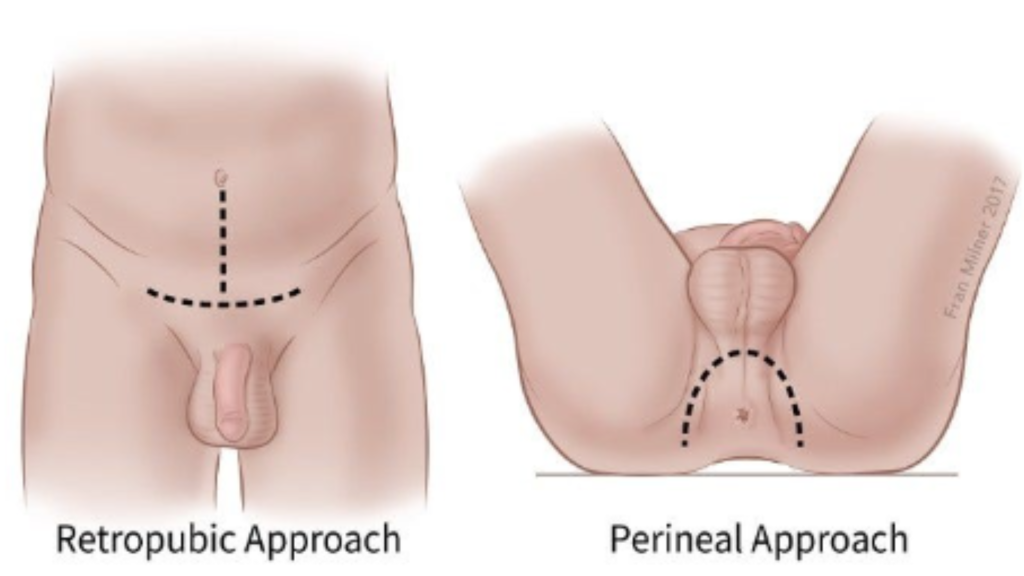
Open radical retropubic vs perineal prostatectomy


Laparoscopic radical prostatectomy through key-hole incisions on the abdomen


Robotic radical prostatectomy done through key-hole incisions on the abdomen assisted by a computer
Objectives and surgical outcome of radical prostatectomy:
The objectives of Radical Prostatectomy is to remove all cancerous tissue from the prostate and the surrounding lymph nodes when necessary, with the primary objective to treat the disease and achieve cure. It is considered a definitive treatment option for localized prostate cancer.
It allows for a histopathological diagnosis and detailed examination of the prostate to determine how aggressive the cancer is and if it has spread outside the prostate gland. It aims to remove the cancer before it spreads to other parts of the body.
For localised cancer, the 10-year survival rate can be around 85–90%; but this varies based on aggressiveness of the disease, its risk stratification and stage of the disease.
A urinary catheter is kept in place for 5- 7 days following surgery to allow the connection between the bladder and urethra to heal.
Important sequelae and expected side effects of the surgery include:
- Urinary Incontinence: Involuntary leakage is common immediately after removing the catheter, but typically improves over 3–6 months with pelvic floor exercises, with most men achieving good control. In some cases, the incontinence may be permanent and requires further intervention
- Erectile Dysfunction: The ability to have erections is often affected. Recovery can take up to two years and depends on whether a “nerve-sparing” technique was possible.
- Dry ejaculation: The procedure cuts the connection for ejaculation, resulting in “dry” orgasms.
SURGERY: OPEN VS LAPAROSCOPIC VS ROBOTIC RADICAL PROSTATECTOMY
As medical professionals, we must critically analyze evidence-based approaches to provide a detailed, informed explanation prior to surgery, and offer them the various approaches.
The choice between open, laparoscopic, and robotic-assisted surgery involves balancing tactile feedback, precision, and recovery speed.
Cancer Control (Oncologic Efficacy)
- Efficacy: Research consistently shows that for most major cancers (such as prostate or kidney), all three methods achieve equivalent oncologic outcomes. Long-term survival rates and cancer-free margins do not significantly differ based on the surgical approach, provided the surgeon is highly skilled in that specific technique.
- Visibility: Robotic and laparoscopic methods offer high-definition, 3D magnification, which can help in visualizing delicate nerves and vessels during tumor removal.
Side Effects and Recovery
- Open Surgery: Requires a large incision, leading to more significant postoperative pain, higher blood loss, and a longer hospital stay. There is a higher risk of wound infections and incisional hernias.
- Laparoscopic/Robotic: These “keyhole” surgeries involve small incisions, resulting in:
- Reduced blood loss and fewer transfusions.
- Less pain and decreased reliance on opioids.
- Faster recovery and shorter hospital stays.
- Lower risk of external scarring and infection.
Several landmark clinical trials have compared these surgical approaches. While individual techniques differ, the consensus across these trials is that oncological outcomes (cancer control) by skilled surgeons are EQUIVALENT, whereas perioperative and functional outcomes may favor robotic approaches.
Key Clinical Trials
| Trial Name | Location | Primary Comparison | Major Findings |
| The Brisbane Trial (Yaxley et al.) | Australia | Open vs. Robotic | First major RCT. Found no difference in cancer control at 2 years. Robotic had less pain and shorter hospital stays. |
| LAPPRO Trial | Sweden | Open vs. Robotic | Large prospective study. Robotic showed lower rates of incontinence and better erectile function recovery at 8 years. |
| São Paulo Trial | Brazil | Open vs. Robotic | Second major RCT. Confirmed equivalent cancer control but noted slightly better early functional recovery in robotic patients. |
| ROSE Trial | Germany | Laparoscopic vs. Robotic | Focused on minimally invasive techniques. Found robotic surgery resulted in lower positive surgical margins in some cases. |
Detailed Comparison of Efficacy and Side Effects
1. Cancer Control (Efficacy)
- Equivalent Survival: All trials show no significant difference in biochemical recurrence (PSA rising) or long-term survival between the three methods.
- Surgical Margins: Robotic surgery sometimes shows slightly lower positive surgical margin (PSM) rates due to 10x magnification and 3D visualisation, which helps the surgeon avoid cutting into the tumor.
2. Side Effects (Functional Outcomes)
- Urinary Continence: Most trials indicate that robotic patients regain control faster than open surgery patients, though long-term results (at 2+ years) tend to equalize.
- Erectile Function: Robotic surgery allows for more precise nerve-sparing. Trials like LAPPRO suggest a significant advantage for robotic surgery in preserving potency compared to open surgery.
3. Perioperative Outcomes (Recovery)
- Blood Loss: Significantly lower in Laparoscopic and Robotic compared to Open.
- Pain & Hospital Stay: Minimally invasive approaches (Robotic / Laparoscopic) consistently lead to less post-op pain and a return to work in 1–2 weeks, vs. 4–6 weeks for Open.
Justifications for Choice of surgery for Prostate Cancer
- Open Surgery: Justified for very large or complex tumors that involve major blood vessels, or for patients with extensive previous abdominal surgeries where scar tissue (adhesions) makes camera navigation dangerous.
- Laparoscopic: A cost-effective alternative to robotics that still offers minimally invasive benefits, though it has a steeper learning curve for the surgeon due to “straight-stick” instruments.
- Robotic (e.g., Da Vinci): Justified by superior dexterity. The “wristed” instruments allow for precise suturing and dissection in tight spaces (like the deep pelvis), making it the gold standard for procedures like radical prostatectomies.
Note: Regardless of the trial data, the experience of the surgeon remains the single most important factor for success, and not the newer modalities of treatment.
Senior urologists critically often use these trial results to tailor the surgical approach to the patient’s specific anatomy and cancer grade.
LAPAROSCOPIC VS ROBOTIC RADICAL PROSTATECTOMY
The debate between Laparoscopic (LRP) and Robotic (RARP) radical prostatectomy centers on several pivotal clinical trials and systematic reviews. While both are minimally invasive, the robotic approach generally shows a slight edge in functional recovery.
Clinical trials and meta-analyses comparing robotic-assisted (RARP) and conventional laparoscopic (LRP) radical prostatectomy generally show equivalent oncological outcomes but superior functional and perioperative results for RARP, such as reduced blood loss, shorter hospital stays, and improved early continence. While many studies are retrospective, prospective trials are accumulating.
Key Trials and Evidence
LAP-01 Trial (NCT03682146): The LAP-01 trial is a notable multicenter, prospective, randomised, patient-blinded controlled trial comparing RARP and LRP, with 782 patients.
Primary Outcome: Time to continence restoration at 3 months.
Secondary Endpoints: Erectile function, quality of life (EORTC-QLQ-C30/PR25), and oncological outcomes up to 3 years.
Systematic Reviews / Meta-Analyses of Trials: Meta-analyses show RARP and LRP are similar in positive surgical margins (PSM) and biochemical recurrence, but RARP shows higher rates of continence and erectile function recovery at 1, 3, 6, and 12 months postoperatively.
Comparative Evidence (RARP vs. LRP):
Operative Time & Stay: RARP typically has shorter operative times (154.9 vs. 169.2 min) and shorter hospital stays (2.3 vs. 3.9 days).
Complications: RARP is associated with lower blood loss, lower transfusion rates, and lower overall complication rates.
Functional Outcomes: RARP often provides better urinary continence and potency recovery compared to LRP.
Major Clinical Trials
- LAP-01 Trial (Germany): This multicenter, randomised trial (782 patients) found that RARP significantly improved potency at 3, 6, and 12 months for nerve-sparing patients. While RARP patients had better early continence, the difference was no longer statistically significant after one year.
- ROSE Trial: Focused on the learning curve and precision, suggesting that RARP may lead to lower positive surgical margin (PSM) rates in advanced stages because of superior 3D magnification and wristed instruments.
- LAPPRO Study (Sweden): While often used to compare open vs. robotic, its data on minimally invasive techniques confirms that RARP generally leads to shorter hospital stays and fewer complications compared to standard laparoscopic or open methods.
Comparative Outcomes
| Feature | Laparoscopic (LRP) | Robotic (RARP) |
| Cancer Control | Equivalent to robotics. | Equivalent to laparoscopic; potentially lower BCR. |
| Potency | Slower recovery of function. | Superior nerve-sparing and faster recovery. |
| Continence | Good long-term results. | Faster early recovery; equivalent at 12 months. |
| Operative Time | Generally longer. | Generally shorter due to better dexterity. |
| Cost | More cost-effective. | Higher initial and maintenance costs. |
Key Findings
- Oncologic Efficacy: Most meta-analyses (e.g., Okegawa et al., Ma et al.) show that both methods are equally effective at removing the cancer, though RARP may reduce the risk of biochemical recurrence (BCR).
- Functional Recovery: The robotic approach is favored for preserving sexual function and achieving earlier urinary control.
- Surgeon Skill: The “learning curve” for robotic surgery is shorter, allowing surgeons to achieve high-precision outcomes more consistently than with traditional “straight-stick” laparoscopy.
Key Takeaways from Comparative Studies of Robotic vs Laparoscopic radical prostatectomy
Robotic assisted radical prostatectomy is generally seen as having a less steeper learning curve, allowing it to surpass conventional Laparoscopic radical prostatectomy in precision and short-term recovery, though it does not show superior long-term cancer control over well-executed conventional laparoscopy.
The conclusions is that the skilled surgeon matters most. While the technology is advanced and provides superior precision, it is a tool operated directly by the surgeon, meaning its success depends heavily on the surgeon’s training, experience, and judgment. The robot enhances human capability but cannot replace human expertise. The surgeon is the one who makes critical decisions during the surgery, and handling unexpected issues, such as anatomic anomalies or patient instability.
The proficiency of the surgeon and the team with the technology greatly affects the efficiency and safety of the procedure.
VERDICT IN 2026
Currently 2026 emphasises a nuanced approach based on disease stage and risk group. Surgery for prostate cancer remains a standard treatment for localised high-risk disease, but its role in advanced disease is being redefined by modern imaging and molecular advancements
Based on research presented at the recent 2026 European Association of Urology (EAU) and ASCO GU meetings, radical prostatectomy in 2026 is increasingly used for high-risk and oligometastatic (low volume metastatic) prostate cancer, supported by precise PSMA PET/CT imaging to improve oncological control. New data highlights its evolving role in personalised medicine, particularly regarding metastatic disease and quality of life.
Key Findings on Radical Prostatectomy in 2026:
Role in Low-Volume Metastatic (Oligometastatic) Hormone Sensitive Prostate Cancer (mHSPC):
Following the TRoMbone feasibility trial (Testing Radical Prostatectomy in Men with Oligometastatic Prostate Cancer that has Spread to the Bone), The PRESIDENT trial (2026) (PRostatEctomy Surgery in Disseminated Low-Volume Metastatic Hormone Sensitive Prostate Cancer with Endpoint Assessment Using Nuclear Imaging Technology Using PSMA PET/CT Imaging) is being enrolled for the use of radical prostatectomy to improve oncological control and reduce local complications compared to radiotherapy in patients with low-volume hormone-sensitive metastatic prostate cancer.
Oligometastatic Disease Strategy:
In the recent 2026 European Association of Urology (EAU) annual meeting, data presented in 2026 reaffirms that in selected patients (e.g., young, low metastatic burden), Radical Prostatectomy combined with systemic therapy results in lower 5-year cancer-specific mortality (13%) compared to systemic therapy alone (23%).
- Radical prostatectomy is a safe option in oligometastatic HSPC as part of a clinical trial
- The evidence for radiotherapy is clearly more solid, yet radical prostatectomy can be an option in selected patients after respective counseling
- In a patient who is young with low metastatic burden, locally resectable disease, and with lower urinary tract symptoms, radical prostatectomy is a reasonable option by inclusion into current trials
High-Risk Localised Disease Management:
While surgery works well for low / intermediate risk, 2026 data shows that high-risk cases (ISUP grade 3–5) benefit significantly from extended pelvic lymph node dissection during RP, improving biochemical recurrence-free survival (10-year data).
In the recent 2026 European Association of Urology (EAU) annual meeting, a 10-year follow-up of a phase 3 trial assessing extended versus limited pelvic lymph node dissection during radical prostatectomy for intermediate- and high-risk prostate cancer presented the following take-home points:
- This long-term randomized phase 3 trial did not demonstrate oncologic superiority of extended pelvic lymphadenectomy over limited pelvic lymphadenectomy in unselected intermediate- and high-risk prostate cancer
- However, in patients with biopsy ISUP grade 3–5, long-term follow-up showed a significant benefit in biochemical recurrence-free survival and metastasis-free survival, suggesting that extended pelvic lymphadenectomy should be the standard of care in this subgroup undergoing radical prostatectomy
Neoadjuvant Therapy Advancements:
Trials are testing neoadjuvant hormonal therapies (e.g., LHRH agonists + darolutamide) before surgery to downstage tumor size and improve surgical resection success in high-risk patients.
COACTION, a randomized trial of neoadjuvant leuprorelin, darolutamide, or both prior to radical prostatectomy for intermediate or high risk prostate cancer, is currently being enrolled.
Adjuvant Therapy Verdict:
The 2026 data confirms that immediate adjuvant therapy (e.g., leuprorelin) after Radical Prostatectomy in patients with undetectable PSA does not improve survival compared to observation but reduces quality of life.
The Randomised Phase 3 AFU-GETUG-20 Trial on leuprorelin treatment immediately after radical prostatectomy in high-risk non-metastatic Prostate Cancer patients with an undetectable PSA level does not improve survival, but increases adverse events, leading to poorer quality of life compared with observation.
Post-Surgery Management:
In the recent EAU 2026 Annual Congress, it was emphasise that for high-risk biochemical recurrence (rising PSA after surgery), treatment with enzalutamide +/- ADT (Androgen Deprivation Therapy) is standard, particularly if the PSA doubling time is 9 months.
- In general, high-risk biochemical recurrences are those that are associated with a PSA doubling time (PSADT) less than 1 year or occurring in patients with pathologic ISUP Grade Group 4-5 disease. Conversely, following radiotherapy, high-risk features include an interval of less than 18 months to biochemical failure or biopsy ISUP Grade Group 4-5 disease.
- In the EMBARK study, prostate cancer patients who had evidence of high-risk disease was defined as PSADT less than 9 months and a PSA level of more than 2 ng per milliliter above nadir following radiation therapy; or more than 1 ng per milliliter after radical prostatectomy, with or without postoperative radiation therapy.
- The EMBARK Phase 3 study showed that enzalutamide (Xtandi) plus leuprolide significantly improves metastasis-free survival (MFS) and overall survival (OS) in high-risk biochemical recurrence (BCR) prostate cancer compared to leuprolide alone. It also demonstrated that enzalutamide monotherapy is more effective than leuprolide alone, but shows no overall survival benefit and leads to earlier therapy re-start.
- Enzalutamide + leuprolide (ADT) reduced the risk of metastasis or death by 58% compared to leuprolide alone.
Conclusions of the 2026 Reviews:
Radical prostatectomy (surgery for prostate cancer) remains a safe and highly effective option for localised and selected low-volume metastatic diseases, with the 2026 focus shifting toward refining patient selection through advanced imaging (PSMA PET/CT) and using neoadjuvant, or prior, therapy to improve long-term outcomes