An Evidence Based Approach In Prostate Cancer Treatment
As medical professionals, our patient management should be evidence-based, not on hearsay or public social media discourse.
Evidence-based medicine is the conscientious, explicit, and judicious use of the current best evidence in making decisions about the care of individual patients.
Evidence-based medicine relies on more than just published studies in peer reviewed journals; it should be based on a critical analysis of evidence and the actual effectiveness of the treatment.
Evidence-Based Medicine relies on three core pillars that, when integrated, ensure high-quality patient care: The best available clinical evidence (from systematic research), the clinician’s expertise and judgement; and the patient’s values, preferences, and unique circumstances. Evidence-Based Medicine is the integration of these components to inform decisions, rather than relying solely on research or intuition.
While efficacy refers to the performance of an intervention under the optimised conditions of a clinical trial, effectiveness evaluates its performance within a real-world clinical setting.
For this, a critical analyses of the various landmark studies is essential to ensure that the most effective management is delivered in prostate cancer treatment.
Localised prostate cancer
Clinical Trials Comparing Active Surveillance (AS), Radical Prostatectomy (RP) And Radiotherapy (RT) In Localised Prostate Cancer
Major clinical trials have compared active surveillance (AS), radical prostatectomy (RP), and radiation therapy (RT) for localised prostate cancer. The consensus across high-level evidence is that while surgery and radiation reduce disease progression, overall survival rates remain extremely high and nearly identical across all three approaches for low- to intermediate-risk patients.
1. The ProtecT Trial (UK)
This is the most definitive trial comparing all three modalities directly.
- Participants: 1,643 men with localised prostate cancer randomized to AS, RP, or RT.
- 15-Year Survival: Prostate cancer-specific survival was approximately 97% regardless of the treatment assigned. There was no significant difference in mortality between the three groups.
- Disease Progression: Men on AS had double the rate of disease progression and metastasis (approx. 9%) compared to those who had surgery or radiation (approx. 5%). However, this did not translate to a difference in survival within the 15-year window.
- Quality of Life: RP led to higher rates of urinary incontinence and sexual dysfunction; RT led to more bowel-related side effects.
2. The PIVOT Trial (USA)
Focused on comparing surgery to “observation” (similar to watchful waiting).
- Findings: Radical prostatectomy did not significantly reduce all-cause or prostate cancer-specific mortality compared to observation over a 10-year median follow-up.
- Subgroup Benefit: Men with a PSA > 10 ng/mL or higher-risk tumors showed a potential survival benefit from surgery, whereas low-risk patients did not.
3. The SPCG-4 Trial (Scandinavia)
A long-term trial comparing surgery to watchful waiting (not modern active surveillance).
- Findings: Surgery significantly reduced both overall mortality and the risk of metastasis.
- Age Factor: The benefit was most pronounced in men under age 65. In older men, the survival difference was negligible, highlighting the importance of life expectancy in treatment decisions.
Summary of Outcomes
| Outcome | Active Surveillance | Radical Prostatectomy | Radiation Therapy |
| 15-Year Survival | Very High (~97%) | Very High (~97%) | Very High (~97%) |
| Metastasis Risk | Slightly Higher | Lower | Lower |
| Main Side Effects | Minimal (psychological stress) | Incontinence, Erectile Dysfunction | Bowel urgency, Erectile Dysfunction |
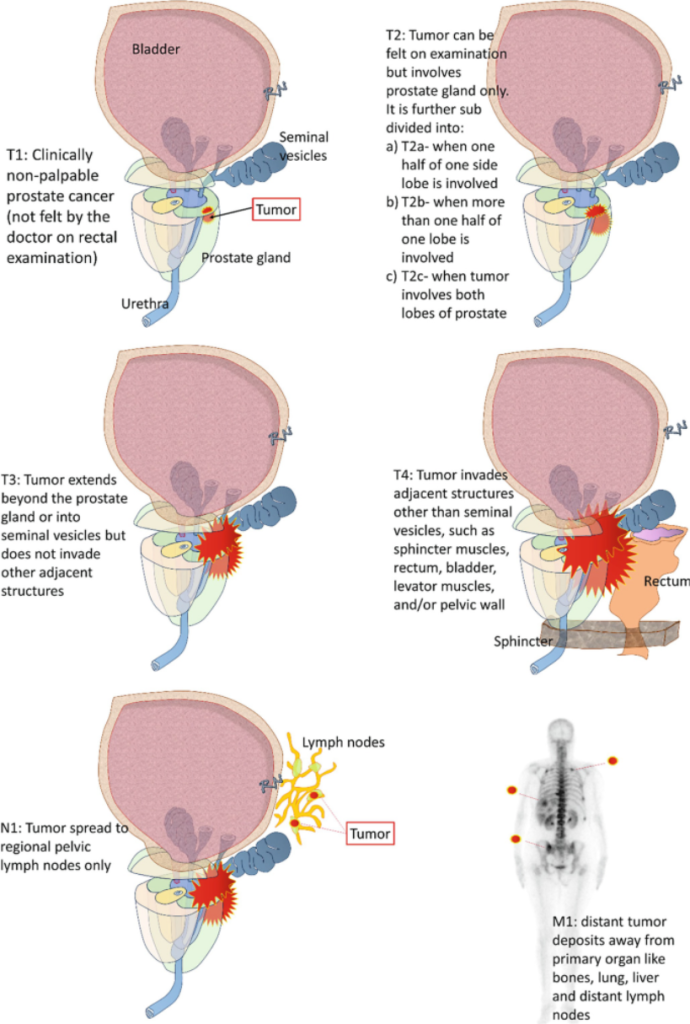
TNM staging of prostate cancer
Risk stratification of prostate cancer – decision on Radical prostatectomy vs Radiotherapy
Risk stratification of prostate cancer – decision on Multimodality approach Radical prostatectomy and Radiotherapy in high risk prostate cancer
Summary Of The Clinical Trials And The Controversies On Observation Versus Active Surveillance Versus Radical Prostatectomy (RP) And Radiotherapy (Rt) In Localised Prostate Cancer
The debates surrounding clinical trials for localised prostate cancer management—specifically comparing Observation / Active Monitoring, Active Surveillance (AS), Radiotherapy (RT), and Radical Prostatectomy (RP) – are among the most intense in Urological oncology.
The controversy stems from a central paradox: curative treatments significantly reduce cancer spread but do not significantly increase long-term survival for most men with localised disease.
1. The Survival vs. Progression Paradox (The “ProtecT” Controversy)
The ProtecT trial (15-year results) is the primary source of debate.
- The Conflict: 15-year prostate cancer-specific survival is nearly identical (~97%) across surgery, radiation, and monitoring. However, those on monitoring had double the risk of metastasis (nearly 10% vs. 5%).
- The Debate: Is avoiding the side effects of surgery / radiation worth a 5% higher risk of incurable metastasis? Critics argue that 15 years is still “too short” for younger men, as the metastatic group will eventually face higher mortality. Proponents argue that the trial proves we are over-treating men who would have died with their cancer rather than of it.
2. Active Monitoring vs. Modern Active Surveillance
- The Conflict: Older trials (ProtecT, PIVOT, SPCG-4 trials) used “Active Monitoring” or “Watchful Waiting,” which were often reactive (waiting for symptoms).
- The Controversy: Modern Active Surveillance (AS) is far more rigorous, using serial MRIs and genomic testing. Experts argue that the “high progression rates” seen in the ProtecT monitoring arm are outdated and do not reflect the safety of modern AS.
3. The “Old World” vs. “New World” trial results (SPCG-4 vs. PIVOT / ProtecT)
There is a stark contradiction between the Scandinavian SPCG-4 trial and the American / British trials (PIVOT / ProtecT trials).
- SPCG-4 found a massive survival benefit for surgery.
- PIVOT / ProtecT found almost no survival benefit for surgery.
- The Controversy: The difference is likely due to PSA screening. SPCG-4 patients were diagnosed in the pre-PSA era with “palpable” (more aggressive) tumors. Critics argue that surgery is vital for “clinically detected” tumors but perhaps unnecessary for “PSA-detected” (screen-detected) tumors.
4. Risk Stratification Failures
- The Conflict: Trials often lump “low-risk” and “intermediate-risk” patients together.
- The Debate: Sub-analyses of PIVOT suggest that men with a PSA > 10 ng/mL or intermediate-risk disease do see a survival benefit from surgery. The controversy lies in the “grey zone”: the intermediate-risk patient (Gleason 7). Some guidelines now favor surgery for these men, while others argue AS is still safe.
5. Quality of Life (QoL) Trade-offs
- The Conflict: Surgery and radiation have distinct “harm profiles.”
- The Controversy:
- Surgery: Immediate hit to urinary continence and sexual function, which may partially recover.
- Radiation: Gradual decline in sexual function and late-onset bowel / bladder irritation (proctitis).
- The Argument: Since survival is the same, many argue Patient-Reported Outcome Measures (PROMs) should be the primary deciding factor.
Summary of the Controversy Matrix
| Trial | Controversy Focus | Verdict of Critics |
| ProtecT | Metastasis vs. Survival | “Monitoring is dangerous because metastasis eventually kills.” |
| PIVOT | Low-risk Overtreatment | “Surgery for PSA < 10 is essentially a placebo for survival.” |
| SPCG-4 | Relevance to Modern Era | “These results only apply to large, aggressive tumors, not today’s cases.” |
| All Trials | Technological Lag | “Trials use open surgery / 3D-conformal RT; they don’t reflect Robotic (RARP) or Proton/SBRT results.” |
In short, the controversy remains: Are we curing patients, or are we simply documenting the slow progression of a disease that wouldn’t have killed them anyway? Most modern specialists, especially senior experienced urologists and oncologists, now use these trials to advocate for a “risk-stratified” approach – AS for low-risk and aggressive “triplet therapy” for higher-risk cases.
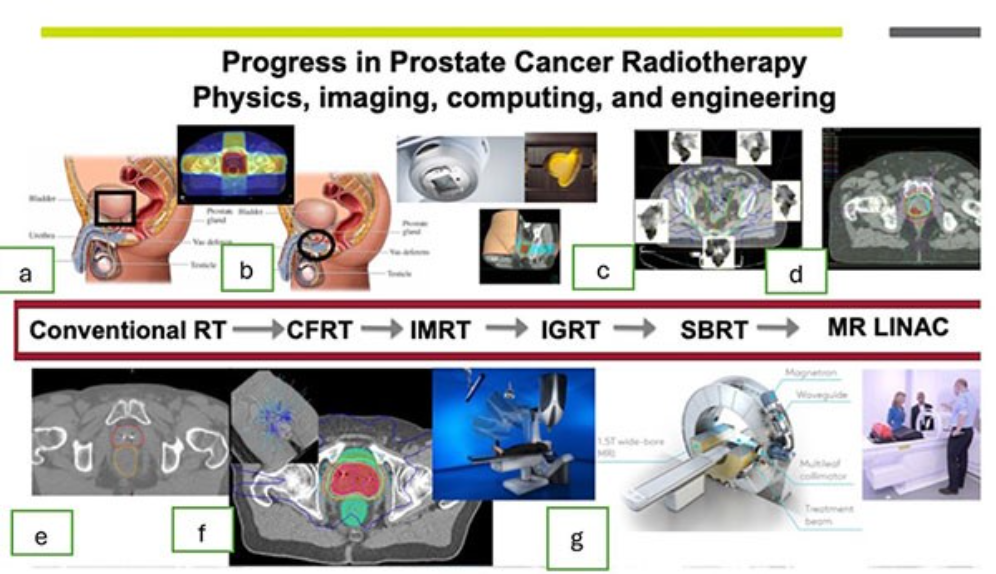
Landmark clinical trials that have moulded the role of radiotherapy in prostate cancer
Landmark radiotherapy trials in prostate cancer have redefined standards by establishing that adding radiation to standard therapy improves survival in low-volume metastatic disease (STAMPEDE) and optimising delivery through shortened courses (hypofractionation).
Key trials include HYPRO (fractionation), POP-RT (pelvic node treatment), and EORTC 22863 (combined with hormone therapy).
Key Landmark Trials for Radiotherapy in Prostate Cancer
STAMPEDE (H arm – Radiotherapy arm): Demonstrated that radiotherapy to the prostate improves overall survival for men with low-volume metastatic prostate cancer, transforming it into a new standard of care.
POP-RT Study: A randomised phase 3 trial showing that prophylactic pelvic node radiotherapy WP-RT (whole pelvic radiotherapy) significantly improves 5-year biochemical relapse-free survival in high-risk prostate cancer, as compared with PO-RT (prostate-only radiotherapy), but overall survival did not appear to differ.
HYPRO Trial (2016): Evaluated hypofractionated radiotherapy (19 fractions of 3.4 Gy) compared with conventionally fractionated radiotherapy (39 fractions of 2.0 Gy), demonstrating comparable outcomes, and supporting shorter treatment schedules.
Scandinavian Hypo Study (HYPO-RT-PC): Compared ultra-hypofractionated (five fractions over one week) radiotherapy to conventional radiotherapy, showing that shorter courses can be safe and equally effective.
EORTC 22863: A seminal trial that established the necessity of combining hormone therapy (3 years) with radiotherapy for high-risk localised prostate cancer, proving improved disease-free and overall survival.
TRANSFORM (2025) – For oligometastasis on the use of SBRT as a metastasis-directed therapy (MDT) for patients with oligometastatic prostate cancer: Published 5-year outcomes confirming that stereotactic body radiotherapy (SBRT) provides durable disease control in oligometastatic prostate cancer.
RADIODOSE & PSMA Trials: Emerging evidence regarding radiotherapy and targeted radiopharmaceuticals (177Lu-PSMA) for advanced, castrate-resistant, or metastatic cases.
Usage Examples and Clinical Practice Implications
Pelvic Treatment: High-risk patients are now treated with pelvic radiotherapy based on the POP-RT study to prevent lymph node recurrence.
Shorter Treatment Times: Treatment is often reduced from 7-8 weeks (37+ sessions) to 4 weeks (20 sessions) or less, based on trials showing equivalence.
Metastatic Management: Radiotherapy is no longer just for localised disease; STAMPEDE supports its use in low-volume metastatic cancer (spread to the prostate only or nearby lymph nodes).
Landmark clinical trials comparing radical prostatectomy with radiotherapy in prostate cancer
There are problems conducting clinical trials comparing radical prostatectomy with radiotherapy in prostate cancer for the following reasons:
- Treatment techniques have evolved over time – namely robotic surgery and advanced radiotherapy techniques including targeted delivery and dose escalation – therefore results are not generalisable to contemporary practice.
- Also there is an inherent difference in the biochemical recurrence criteria after radiation therapy vs radical prostatectomy.
- High-level comparative evidence regarding surgery versus radiation-based treatment for high-risk Prostate Cancer is lacking.
Landmark clinical trials and prospective studies comparing radical prostatectomy (RP) with radiotherapy (RT) in prostate cancer have largely established that both treatments offer similar long-term cancer-specific survival for localised disease, though they differ significantly in toxicity and quality-of-life outcomes.
Key trials and comparative studies include:
1. The ProtecT Trial (2016/2023)
Significance: The largest randomized controlled trial comparing active monitoring, radical prostatectomy, and external beam radiotherapy (EBRT) for screen-detected localised prostate cancer.
Key Findings: After 10 years, there was no significant difference in prostate cancer-specific mortality (PCSM) among the three groups.
Outcome: Established equipoise (equivalent effectiveness) between surgery and radiotherapy for low to intermediate-risk prostate cancer.
At a median of 10 years, prostate-cancer-specific mortality was low irrespective of the treatment assigned, with no significant difference among treatments. Surgery and radiotherapy were associated with lower incidences of disease progression and metastases than was active monitoring, but no difference in overall survival.
2. The PIVOT Trial (2017)
Significance: Compared radical prostatectomy with watchful waiting.
Key Findings: While not a direct RP vs. RT trial, PIVOT showed that for low-risk disease, surgical removal did not improve survival over observation. It indicated that in the modern PSA era, early localized prostate cancer has low mortality regardless of initial treatment type.
3. PACE-A Trial (2024)
Significance: The first phase III randomised trial comparing stereotactic body radiotherapy (SBRT) with surgery (specifically robotic prostatectomy) in localized, intermediate-risk prostate cancer.
Key Findings: SBRT was associated with less patient-reported urinary incontinence and better sexual function at 2 years, while surgery had better bowel function scores.
Outcome: Provided level 1 evidence that SBRT and modern surgery have different, specialized side-effect profiles rather than superior overall efficacy.
4. Scandinavian SPCG-15 Trial (Ongoing)
Significance: A critical ongoing Phase III randomized trial specifically for high-risk prostate cancer / locally advanced prostate cancer patients.
Objective: To compare surgery with modern radiotherapy + Androgen Deprivation Therapy (ADT).
Current Status: Results are highly anticipated to determine if surgery or radiation is superior in the high-risk setting.
High risk prostate cancer / locally advanced prostate cancer
Standard of care treatment options for high-risk prostate cancer include radiation therapy with long-term ADT (NCCN Category 1 recommendation) or radical prostatectomy with selective use of postoperative radiation therapy +/- ADT (NCCN Category 2A recommendation).
Multiple, primarily retrospective, observational studies comparing RP with dose-escalated EBRT and ADT in this patient population have been published.
In the majority of studies, no significant differences in oncological outcomes [e.g. Distant metastasis-free survival (DMFS), Prostate Cancer-Specific Survival (PCSS) and overall survival (OS)] between treatment with RP and EBRT combined with ADT were observed.
Currently, the ‘Scandinavian Surgery Versus Radiotherapy for Locally Advanced Prostate Cancer’ (SPCG-15) trial is the only randomised study comparing RP and EBRT in men with locally advanced Prostate Cancer.
Of the current NCCN guideline recommended treatment regimens, a radiotherapy-based treatment regimen appears to result in a lower incidence of distant metastasis than a surgery-based regimen for patients enrolled in phase III RCTs.
Approximately 80% of men with high risk prostate cancer treated with surgery will receive further treatment or experience recurrence. Adjuvant and early salvage radiotherapy remains critical for this population.
Use of triple or quadruplet therapy of neoadjuvant chemotherapy + ADT, radical prostatectomy, and personalized post-operative radiotherapy + ADT may mitigate these differences when compared to a doublet of radiotherapy + long-term ADT. However, toxicity and cost implications require further study.
SPCG-15 is an actively enrolling phase III trial aimed to directly address this question. Notably, it is a more favorable risk population than the present study.
5. Retrospective / Observational Landmark Studies
Because prospective randomized data comparing RP vs. RT is sparse, large observational studies have heavily influenced practice:
Wenzel et al. (2025): Propensity-score-matched analysis showed no differences between RP and RT in MFS (metastasis-free), CSS (cancer-specific), and OS (overall survival), suggesting equal effectiveness in specialised centers.
Swedish National Study (2014) – Sooriakumaran et al: This large observational study with follow-up to 15 years suggests that for most men with non-metastatic prostate cancer, surgery leads to better survival than radiotherapy. Younger men and those with less comorbidity who have intermediate or high risk localized prostate cancer might have a greater benefit from surgery.
Key Takeaways from Landmark Evidences
Survival: For low and intermediate-risk, both RP and EBRT are equally effective.
Toxicity: RP causes more incontinence and sexual dysfunction; RT causes more bowel issues.
High-Risk: High-risk patients likely benefit more from multimodal treatment (RP+RT or RT+ADT) rather than monotherapy
Verdict in 2026
As of early 2026, the clinical verdict for localized prostate cancer centers on personalized, risk-stratified management rather than a “one-size-fits-all” approach.
Key evidence, including long-term data from trials like the ProtecT Trial indicates that for low- and favorable intermediate-risk group prostate cancers while radical prostatectomy and radiotherapy offer superior biochemical control (less cancer spread), they do not necessarily improve overall survival at 10–15 years compared to active surveillance (AS), and they come with higher rates of sexual, urinary, and bowel side effects.
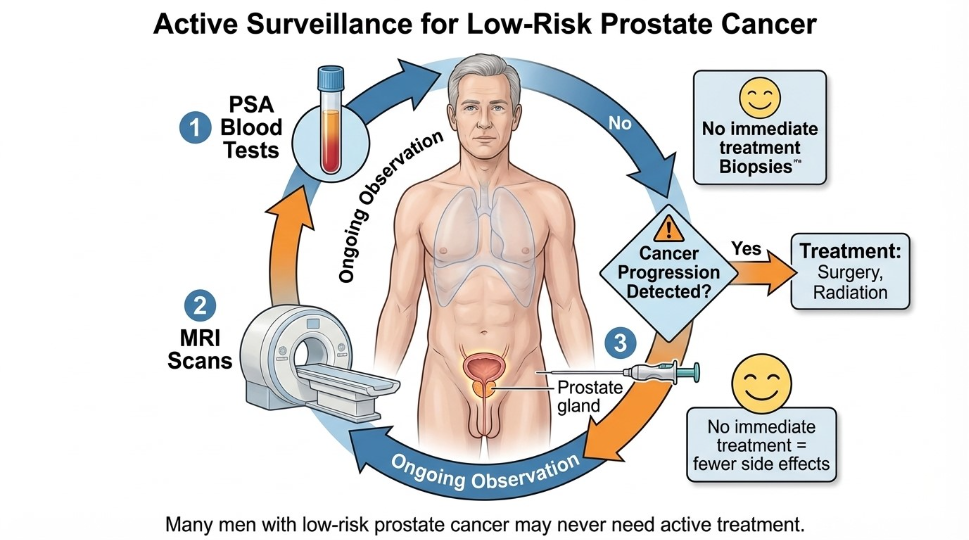
1. Low-Risk Localised Prostate Cancer
Verdict: Active Surveillance is Standard.
Rationale: Active surveillance is the preferred management strategy, providing equivalent 15-year survival to immediate radical treatment while minimising immediate side effects.
2026 Context: MRI-targeted biopsy should be used to confirm risk, but it does not replace the need for surveillance biopsies.
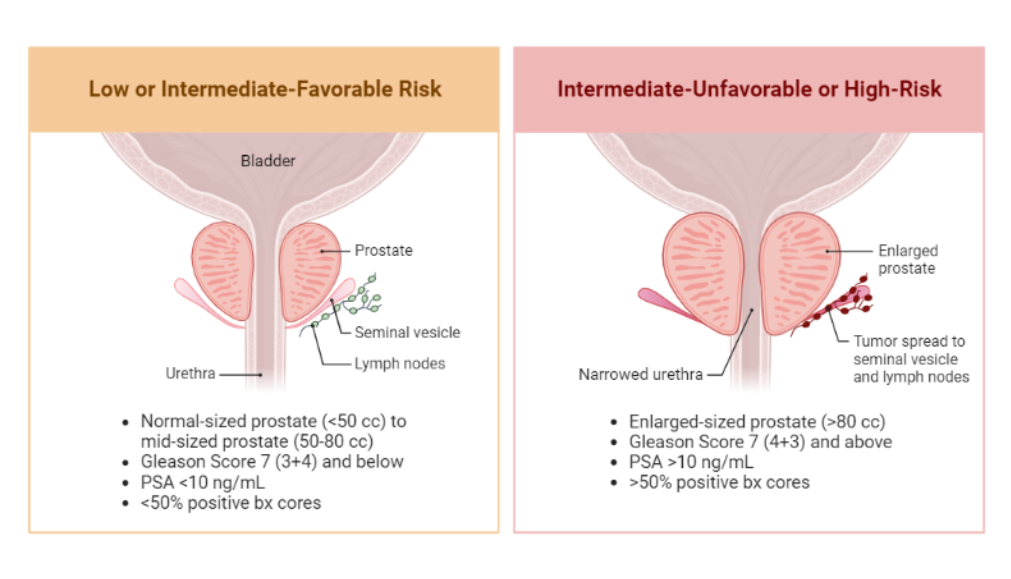
2. Intermediate-Risk Localised Prostate Cancer
Verdict: Risk-Adapted Selection (AS vs. Radical Treatment).
- Favorable Intermediate: Active surveillance is increasingly chosen, especially if the patient is older or prefers to avoid side effects.
- Unfavorable Intermediate: Radical prostatectomy (RARP) or radiotherapy with short-term Androgen Deprivation Therapy (ADT) is typically recommended.
- 2026 Update: The FLAME trial (Focal Lesion Ablative Microboost in prostate cancer) indicates that for intermediate / high risk, adding a focal radiation “boost” to MRI-visible targets improves 5-year biochemical disease-free survival (bDFS) of 92% vs 85%, with a 10-year bDFS of 86% in the focal boost arm vs. 71% in the standard arm.
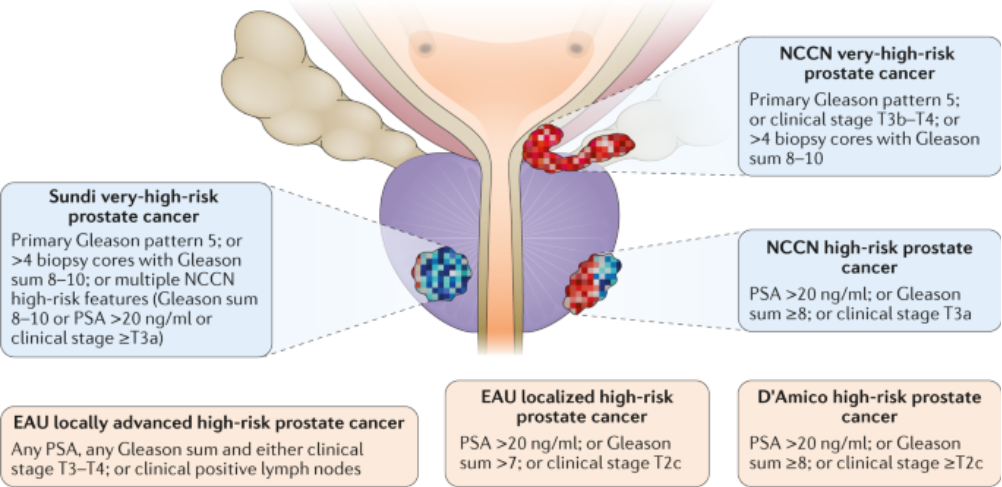
3. High-Risk Localised Prostate Cancer
Verdict: Radical Treatment Required (Surgery or Radiation).
- Approach: Multimodal treatment, often involving radical prostatectomy with lymph node dissection or radiation with long-term ADT.
- 2026 Update: For high-risk prostate cancer, adding androgen receptor signaling inhibitors (like abiraterone + prednisone) to radiotherapy and ADT for 24 months is strongly recommended.
- Comparison: Surgery shows an advantage in cancer-specific mortality over radiotherapy in younger/fitter patients in some high-risk studies, but radiotherapy combined with modern techniques offers similar survival outcomes.
Summary of Comparative Outcomes (2026)
- Survival: No significant difference in 10–15-year survival between radical prostatectomy and modern radiotherapy (like SBRT) for most patients.
- Quality of Life (QoL): Radical prostatectomy (RARP) is associated with higher rates of urinary incontinence and sexual dysfunction.
- Bowel Toxicity: Radiotherapy has a higher, though improved, risk of bowel problems.
- Active Surveillance: Safest choice for low-risk, maintaining best urinary / sexual QoL, but requires strict adherence to monitoring to detect progression.